Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Thomas Jefferson University Hospital, Philadelphia, PA.
Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Yale New Haven Hospital, New Haven, CT.
Am J Obstet Gynecol MFM. 2020 Aug;2(3):100124. doi: 10.1016/j.ajogmf.2020.100124. Epub 2020 Apr 28.
Although the use of 17-alpha-hydroxyprogesterone caproate is one of the most commonly used strategies to reduce the risk of preterm birth since its approval by the Food and Drug Administration in 2011, there has been controversy recently that there may be no benefit associated with its use in singleton pregnancies in women with a prior history of spontaneous preterm birth. However, very few of these investigations evaluated the use of intramuscular progesterone in twin pregnancies. A few studies that used 17-alpha-hydroxyprogesterone caproate in twin pregnancies had mainly included unselected twin pregnancies. Although a twin pregnancy is independently associated with an increased likelihood of preterm birth, the primary indication for the use of supplemental progesterone in pregnancy is prior history of spontaneous preterm birth. Therefore, our investigation of weekly intramuscular progesterone in twin pregnancies with this birth history best addresses this question using a selected cohort.
To assess whether weekly 17-alpha-hydroxyprogesterone caproate prevents recurrent preterm birth in women with a current twin pregnancy and a prior singleton spontaneous preterm birth.
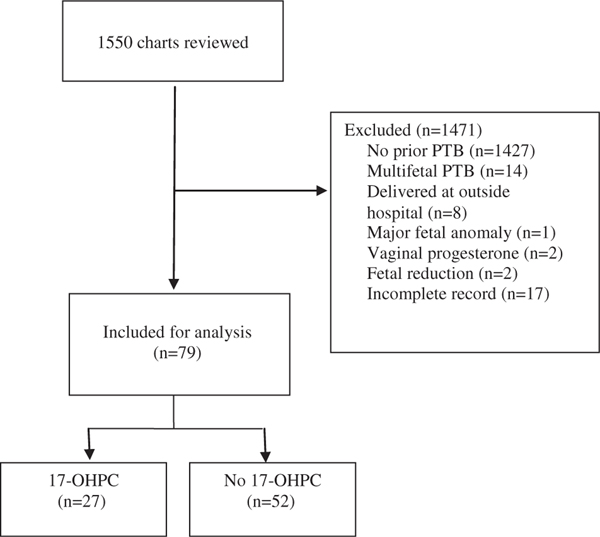
This was a retrospective cohort study of women with twin pregnancy and a prior singleton spontaneous preterm birth in 2 institutions between January 2005 and December 2016. One group (intervention group) consisted of women who received weekly 17-alpha-hydroxyprogesterone caproate, whereas the other (control group) did not. The primary outcome was twin spontaneous preterm birth <34 weeks compared with odds ratio and adjusted odds ratio, adjusting for potential confounders. Secondary outcomes included composite neonatal morbidity such as respiratory distress syndrome, intraventricular hemorrhage, necrotizing enterocolitis, admission to the neonatal intensive care nursery, and fetal or neonatal death before hospital discharge.
A total of 79 patients were included; 27 women received weekly 17-alpha-hydroxyprogesterone caproate and 52 did not. There were no statistically significant differences in maternal demographics except for age. Spontaneous preterm birth <34 weeks occurred in 16 patients (59%) in the intervention group vs 24 (46%) in the control group (odds ratio, 1.69; 95% confidence interval, 0.68-4.54). Composite neonatal morbidity occurred in 20 pregnancies (74%) in the intervention group and 41 pregnancies (79%) in the control group (odds ratio, 0.76; 95% confidence interval, 0.27-2.12). There remained no differences in outcomes after adjusting for potential confounders.
In our study, weekly 17-alpha-hydroxyprogesterone caproate did not prevent spontaneous preterm birth or neonatal morbidity in women with twins and a prior singleton spontaneous preterm birth; however, further research with larger numbers and prospective design is needed.
自 2011 年食品和药物管理局批准 17-α-羟孕酮己酸酯以来,它已成为降低早产风险的最常用策略之一,但最近有争议认为,对于有自发性早产史的单胎妊娠妇女,使用该药物可能没有益处。然而,很少有研究评估其在双胎妊娠中的应用。一些在双胎妊娠中使用 17-α-羟孕酮己酸酯的研究主要包括未选择的双胎妊娠。尽管双胎妊娠本身与早产的可能性增加有关,但妊娠中补充孕激素的主要指征是既往有自发性早产史。因此,我们使用这种具有特定出生史的选定队列,对双胎妊娠中每周肌内注射孕激素进行了研究,以最好地解决这个问题。
评估每周肌内注射 17-α-羟孕酮己酸酯是否能预防有当前双胎妊娠和既往单胎自发性早产史的妇女再次发生早产。
这是 2005 年 1 月至 2016 年 12 月在 2 家机构中进行的一项回顾性队列研究,研究对象为有双胎妊娠和既往单胎自发性早产史的妇女。一组(干预组)接受每周 17-α-羟孕酮己酸酯治疗,另一组(对照组)未接受治疗。主要结局是与比值比和调整比值比相比,双胎自发性早产<34 周,调整了潜在混杂因素。次要结局包括呼吸窘迫综合征、脑室出血、坏死性小肠结肠炎、新生儿重症监护病房入院和出院前胎儿或新生儿死亡等复合新生儿发病率。
共纳入 79 例患者;27 例患者接受每周 17-α-羟孕酮己酸酯治疗,52 例患者未接受治疗。除年龄外,产妇人口统计学特征无统计学差异。干预组有 16 例(59%)发生<34 周自发性早产,对照组有 24 例(46%)(比值比,1.69;95%置信区间,0.68-4.54)。干预组有 20 例(74%)妊娠发生复合新生儿发病率,对照组有 41 例(79%)妊娠发生(比值比,0.76;95%置信区间,0.27-2.12)。在调整了潜在混杂因素后,结果仍无差异。
在我们的研究中,每周肌内注射 17-α-羟孕酮己酸酯并不能预防有双胎妊娠和既往单胎自发性早产史的妇女发生自发性早产或新生儿发病率;然而,需要进行更多数量和前瞻性设计的研究。