Julius Centre for Health Sciences and Primary Care, University Medical Centre Utrecht, Utrecht, the Netherlands; Department of Obstetrics and Gynaecology, Academic Medical Centre Amsterdam, Amsterdam, the Netherlands.
BJOG. 2015 Jan;122(1):27-37. doi: 10.1111/1471-0528.13032. Epub 2014 Aug 22.
In twin pregnancies, the rates of adverse perinatal outcome and subsequent long-term morbidity are substantial, and mainly result from preterm birth (PTB).
To assess the effectiveness of progestogen treatment in the prevention of neonatal morbidity or PTB in twin pregnancies using individual participant data meta-analysis (IPDMA).
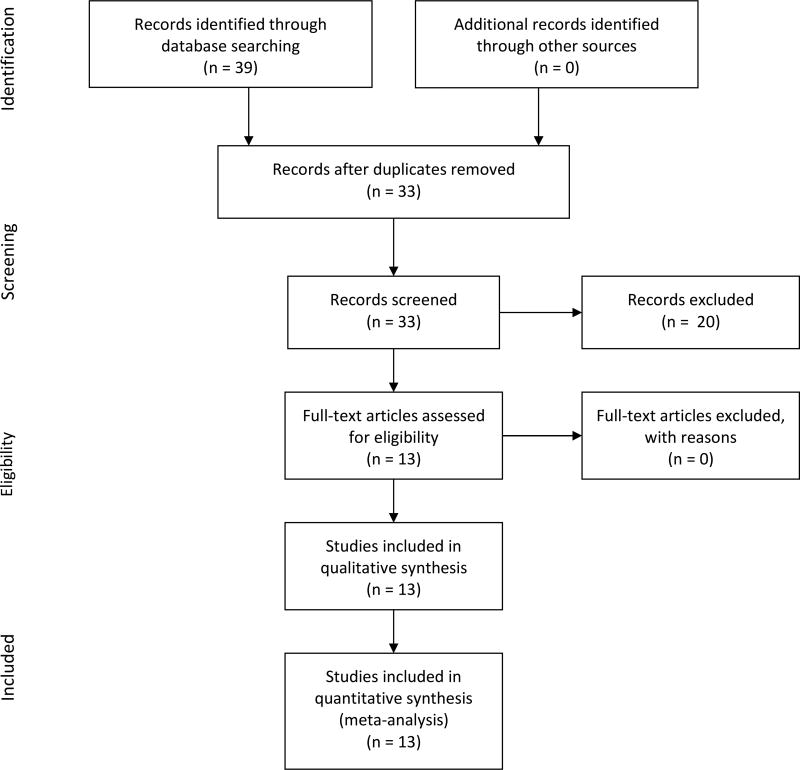
We searched international scientific databases, trial registration websites, and references of identified articles.
Randomised clinical trials (RCTs) of 17-hydroxyprogesterone caproate (17Pc) or vaginally administered natural progesterone, compared with placebo or no treatment.
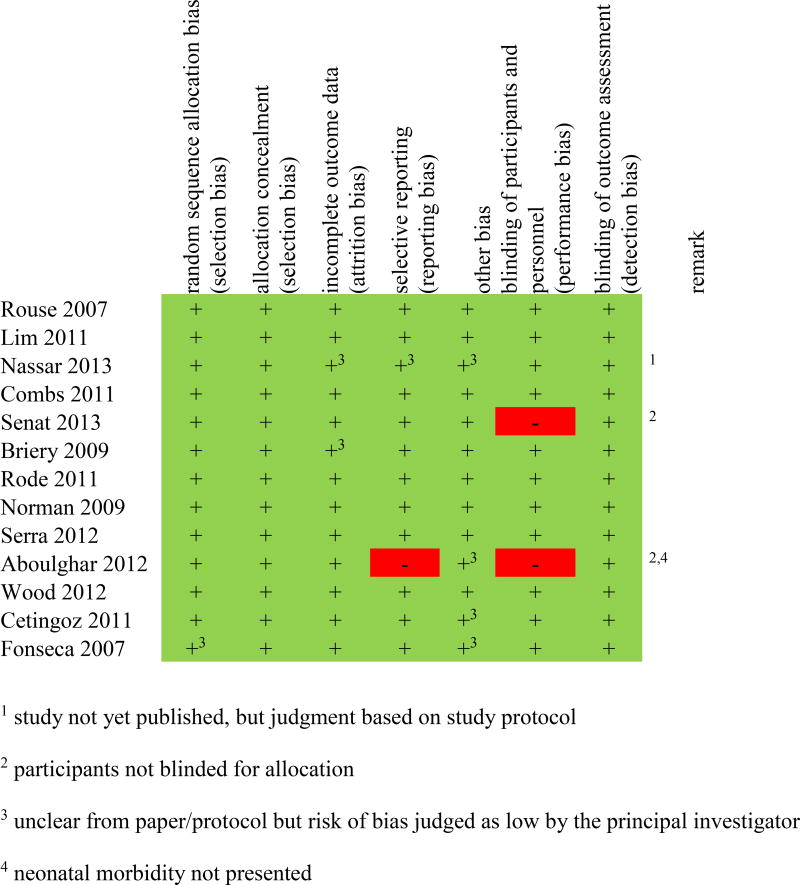
Investigators of identified RCTs were asked to share their IPD. The primary outcome was a composite of perinatal mortality and severe neonatal morbidity. Prespecified subgroup analyses were performed for chorionicity, cervical length, and prior spontaneous PTB.
Thirteen trials included 3768 women and their 7536 babies. Neither 17Pc nor vaginal progesterone reduced the incidence of adverse perinatal outcome (17Pc relative risk, RR 1.1; 95% confidence interval, 95% CI 0.97-1.4, vaginal progesterone RR 0.97; 95% CI 0.77-1.2). In a subgroup of women with a cervical length of ≤25 mm, vaginal progesterone reduced adverse perinatal outcome when cervical length was measured at randomisation (15/56 versus 22/60; RR 0.57; 95% CI 0.47-0.70) or before 24 weeks of gestation (14/52 versus 21/56; RR 0.56; 95% CI 0.42-0.75).
AUTHOR'S CONCLUSIONS: In unselected women with an uncomplicated twin gestation, treatment with progestogens (intramuscular 17Pc or vaginal natural progesterone) does not improve perinatal outcome. Vaginal progesterone may be effective in the reduction of adverse perinatal outcome in women with a cervical length of ≤25 mm; however, further research is warranted to confirm this finding.
在双胞胎妊娠中,不良围产儿结局和随后的长期发病率很高,主要是由于早产(PTB)所致。
使用个体参与者数据荟萃分析(IPDMA)评估孕激素治疗预防双胞胎妊娠新生儿发病率或 PTB 的效果。
我们搜索了国际科学数据库、试验注册网站和已确定文章的参考文献。
17-羟孕酮己酸酯(17Pc)或阴道给予天然孕激素与安慰剂或不治疗的随机对照试验(RCTs)。
要求确定的 RCT 的研究者共享他们的 IPD。主要结局是围产儿死亡率和严重新生儿发病率的综合指标。针对绒毛膜性、宫颈长度和先前自发性 PTB 进行了预设的亚组分析。
13 项试验纳入了 3768 名妇女及其 7536 名婴儿。17Pc 和阴道孕酮均未降低不良围产儿结局的发生率(17Pc 相对风险,RR1.1;95%置信区间,95%CI0.97-1.4;阴道孕酮 RR0.97;95%CI0.77-1.2)。在宫颈长度≤25mm 的女性亚组中,当宫颈长度在随机分组时(15/56 与 22/60;RR0.57;95%CI0.47-0.70)或在 24 孕周之前测量时(14/52 与 21/56;RR0.56;95%CI0.42-0.75),阴道孕酮降低不良围产儿结局。
在无并发症的双胞胎妊娠中,未选择孕激素治疗(肌肉内 17Pc 或阴道天然孕激素)不会改善围产儿结局。阴道孕酮可能对宫颈长度≤25mm 的女性降低不良围产儿结局有效;然而,需要进一步研究来证实这一发现。