Pediatric Epilepsy Program, Massachusetts General Hospital, Boston.
Department of Neurology and Pediatrics, University of Alabama School of Medicine, Birmingham.
JAMA Neurol. 2021 Mar 1;78(3):285-292. doi: 10.1001/jamaneurol.2020.4607.
Efficacy of cannabidiol has been demonstrated in seizures associated with Lennox-Gastaut and Dravet syndromes but appears not yet to have been established in conditions with primarily focal seizures, such as tuberous sclerosis complex (TSC).
To evaluate efficacy and safety of 25-mg/kg/day and 50-mg/kg/day cannabidiol dosages vs placebo against seizures associated with TSC.
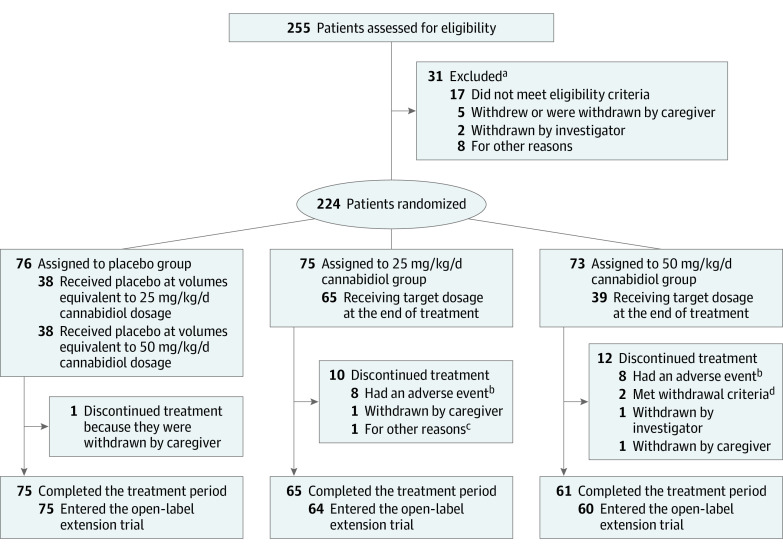
DESIGN, SETTING, AND PARTICIPANTS: This double-blind, placebo-controlled randomized clinical trial (GWPCARE6) enrolled patients between April 6, 2016, and October 4, 2018; follow-up was completed on February 15, 2019. The trial was conducted at 46 sites in Australia, Poland, Spain, the Netherlands, United Kingdom, and United States. Eligible patients (aged 1-65 years) were those with a clinical diagnosis of TSC and medication-resistant epilepsy who had had at least 8 TSC-associated seizures during the 4-week baseline period, with at least 1 seizure occurring in at least 3 of the 4 weeks, and were currently taking at least 1 antiepileptic medication.
Patients received oral cannabidiol at 25 mg/kg/day (CBD25) or 50 mg/kg/day (CBD50) or a matched placebo for 16 weeks.
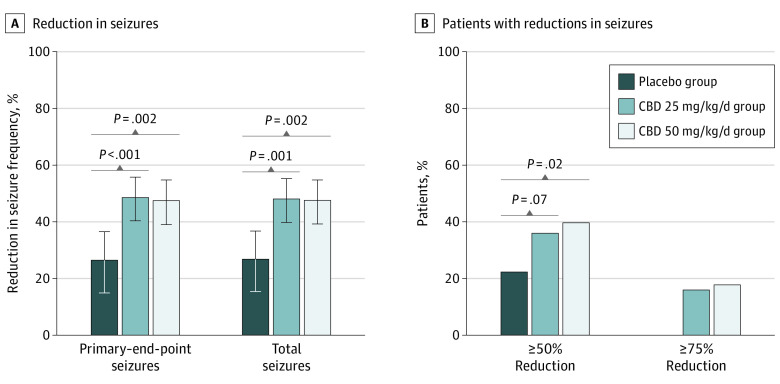
The prespecified primary outcome was the change from baseline in number of TSC-associated seizures for cannabidiol vs placebo during the treatment period.
Of 255 patients screened for eligibility, 31 were excluded and 224 were randomized. Of the 224 included patients (median [range] age, 11.4 [1.1-56.8] years; 93 female patients [41.5%]), 75 were randomized to CBD25, 73 to CBD50, and 76 to placebo, with 201 completing treatment. The percentage reduction from baseline in the type of seizures considered the primary end point was 48.6% (95% CI, 40.4%-55.8%) for the CBD25 group, 47.5% (95% CI, 39.0%-54.8%) for the CBD50 group, and 26.5% (95% CI, 14.9%-36.5%) for the placebo group; the percentage reduction from placebo was 30.1% (95% CI, 13.9%-43.3%; P < .001) for the CBD25 group and 28.5% (95% CI, 11.9%-42.0%; nominal P = .002) for the CBD50 group. The most common adverse events were diarrhea (placebo group, 19 [25%]; CBD25 group, 23 [31%]; CBD50 group, 41 [56%]) and somnolence (placebo group, 7 [9%]; CBD25 group, 10 [13%]; CBD50 group, 19 [26%]), which occurred more frequently with cannabidiol than placebo. Eight patients in CBD25 group, 10 in CBD50 group, and 2 in the placebo group discontinued treatment because of adverse events. Twenty-eight patients taking cannabidiol (18.9%) had elevated liver transaminase levels vs none taking placebo.
Cannabidiol significantly reduced TSC-associated seizures compared with placebo. The 25-mg/kg/day dosage had a better safety profile than the 50-mg/kg/day dosage.
ClinicalTrials.gov Identifier: NCT02544763.
已证明大麻二酚在 Lennox-Gastaut 和 Dravet 综合征相关的癫痫发作中有效,但似乎尚未在主要局灶性癫痫发作的情况下(如结节性硬化症复合征 (TSC))确立其疗效。
评估 25 毫克/公斤/天和 50 毫克/公斤/天的大麻二酚剂量与安慰剂相比,对 TSC 相关癫痫发作的疗效和安全性。
设计、地点和参与者: 这项双盲、安慰剂对照随机临床试验 (GWPCARE6) 于 2016 年 4 月 6 日至 2018 年 10 月 4 日招募患者;随访于 2019 年 2 月 15 日完成。该试验在澳大利亚、波兰、西班牙、荷兰、英国和美国的 46 个地点进行。符合条件的患者(年龄 1-65 岁)为临床诊断为 TSC 和药物难治性癫痫的患者,他们在 4 周基线期内至少有 8 次 TSC 相关癫痫发作,至少有 1 次发作发生在至少 4 周中的 3 周,且目前正在服用至少 1 种抗癫痫药物。
患者接受口服大麻二酚 25 毫克/公斤/天(CBD25)或 50 毫克/公斤/天(CBD50)或匹配的安慰剂治疗 16 周。
预先指定的主要结局是治疗期间大麻二酚与安慰剂相比,TSC 相关癫痫发作的数量从基线的变化。
在 255 名筛选符合条件的患者中,有 31 名被排除在外,224 名被随机分组。在纳入的 224 名患者中(中位数 [范围] 年龄,11.4 [1.1-56.8] 岁;93 名女性患者 [41.5%]),75 名被随机分配至 CBD25 组,73 名至 CBD50 组,76 名至安慰剂组,201 名完成治疗。考虑为主要终点的癫痫发作类型从基线的百分比减少分别为 CBD25 组 48.6%(95%CI,40.4%-55.8%),CBD50 组 47.5%(95%CI,39.0%-54.8%)和安慰剂组 26.5%(95%CI,14.9%-36.5%);与安慰剂相比,CBD25 组减少 30.1%(95%CI,13.9%-43.3%;P < .001),CBD50 组减少 28.5%(95%CI,11.9%-42.0%;名义 P = .002)。最常见的不良事件是腹泻(安慰剂组 19 例 [25%];CBD25 组 23 例 [31%];CBD50 组 41 例 [56%])和嗜睡(安慰剂组 7 例 [9%];CBD25 组 10 例 [13%];CBD50 组 19 例 [26%]),这些不良事件在使用大麻二酚时比安慰剂更常见。CBD25 组 8 例患者、CBD50 组 10 例患者和安慰剂组 2 例患者因不良事件停止治疗。28 名服用大麻二酚的患者(18.9%)的肝转氨酶水平升高,而服用安慰剂的患者则没有。
与安慰剂相比,大麻二酚显著减少 TSC 相关癫痫发作。25 毫克/公斤/天的剂量与 50 毫克/公斤/天的剂量相比具有更好的安全性。
ClinicalTrials.gov 标识符:NCT02544763。