Biosecurity Research Program, The Kirby Institute, UNSW, Wallace Wurth Building, High St, Kensington Campus, NSW 2052, Australia.
School of Public Health and Community Medicine, UNSW, Wallace Wurth Building, High St, Kensington Campus, NSW 2052, Australia.
Int J Nurs Stud. 2021 Feb;114:103811. doi: 10.1016/j.ijnurstu.2020.103811. Epub 2020 Oct 29.
There are no publicly available national data on healthcare worker infections in Australia. It has been documented in many countries that healthcare workers (HCW) are at increased occupational risk of COVID-19. We aimed to estimate the burden of COVID-19 on Australia HCW and the health system by obtaining and organizing data on HCW infections, analyzing national HCW cases in regards to occupational risk and analyzing healthcare outbreak.
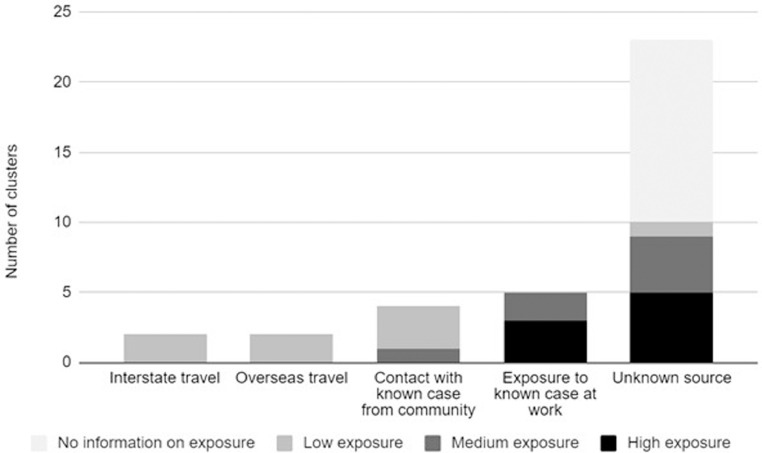
We searched government reports and websites and media reports to create a comprehensive line listing of Australian HCW infections and nosocomial outbreaks between January 25 and July 8, 2020. A line list of HCW related COVID-19 reported cases was created and enhanced by matching data extracted from media reports of healthcare related COVID-19 relevant outbreaks and reports, using matching criteria. Rates of infections and odds ratios (ORs) for HCW were calculated per state, by comparing overall cases to HCW cases. To investigate the sources of infection amongst HCW, transmission data were collated and graphed to show distribution of sources.
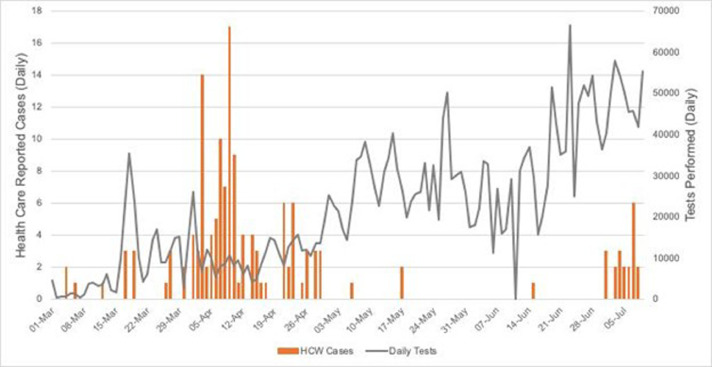
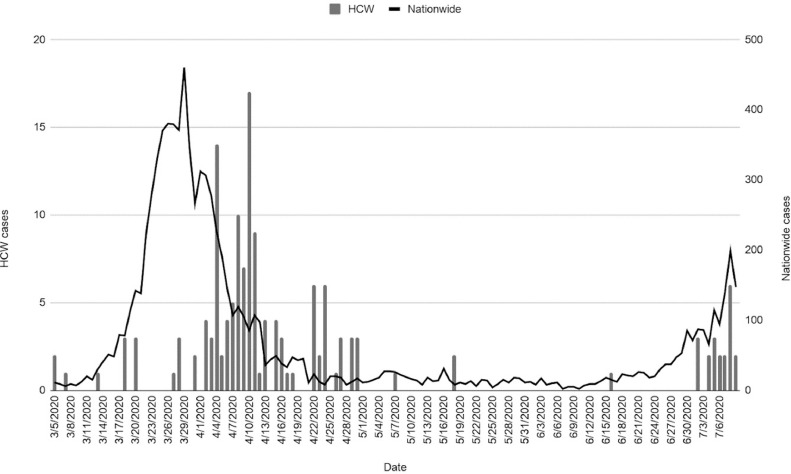
We identified 36 hospital outbreaks or HCW infection reports between January 25 and July 8, 2020. According to our estimates, at least 536 HCW in Australia had been infected with COVID-19, comprising 6.03% of all reported infections. The rate of HCW infection was 90/100000 and of community infection 34/100,000. HCW were 2.69 times more likely to contract COVID-19 (95% CI 2.48 to 2.93; P < 0.001). The timing of hospital outbreaks did not always correspond to community peaks. Where data were available, a total of 131 HCW across 21 outbreaks led to 1656 HCW being furloughed for quarantine. In one outbreak, one hospital was closed and 1200 HCW quarantined.
The study shows that HCW were at nearly 3 times the risk of infection. Of concern, this nearly tripling of risk occurred during a period of low community prevalence suggesting failures at multiple hazard levels including PPE policies within the work environment. Even in a country with relatively good control of COVID-19, HCW are at greater risk of infection than the general community and nosocomial outbreaks can have substantial effects on workforce capacity by the quarantine of numerous HCW during an outbreak. The occurrence of hospital outbreaks even when community incidence was low highlights the high risk setting that hospitals present. Australia faced a resurgence of COVID-19 after the study period, with multiple hospital outbreaks. We recommend formal reporting of HCW infections, testing protocols for nosocomial outbreaks, cohorting of workforce to minimize the impact, and improved PPE guidelines to provide precautionary and optimal protection for HCW.
澳大利亚尚无关于医护人员感染的公开全国数据。许多国家都有记录表明,医护人员(HCW)面临着更高的 COVID-19 职业风险。我们旨在通过获取和整理有关 HCW 感染的数据、分析全国 HCW 病例的职业风险以及分析医疗保健暴发,来估算 COVID-19 对澳大利亚 HCW 和卫生系统的负担。
我们搜索了政府报告和网站以及媒体报道,以创建一份澳大利亚 HCW 感染和医院内暴发的综合清单,时间范围为 2020 年 1 月 25 日至 7 月 8 日。创建了一份 HCW 相关 COVID-19 报告病例的清单,并通过使用匹配标准从与医疗保健相关的 COVID-19 相关暴发和报告的媒体报道中提取数据,对其进行了增强。通过将总病例数与 HCW 病例数进行比较,按州计算了感染率和 HCW 的优势比(OR)。为了调查 HCW 感染的来源,我们收集和绘制了传播数据以显示来源分布。
我们在 2020 年 1 月 25 日至 7 月 8 日期间发现了 36 起医院暴发或 HCW 感染报告。根据我们的估计,澳大利亚至少有 536 名 HCW 感染了 COVID-19,占所有报告感染病例的 6.03%。HCW 的感染率为 90/100000,社区感染率为 34/100000。HCW 感染 COVID-19 的可能性是社区感染的 2.69 倍(95%CI 2.48 至 2.93;P < 0.001)。医院暴发的时间并不总是与社区高峰相对应。在有数据的情况下,21 次暴发中的 131 名 HCW 导致 1656 名 HCW 因隔离而休假。在一次暴发中,一家医院关闭,1200 名 HCW 被隔离。
该研究表明,HCW 的感染风险几乎增加了 3 倍。令人担忧的是,这种风险几乎增加了三倍是在社区患病率较低的时期发生的,这表明在工作环境中的个人防护设备(PPE)政策等多个危险级别都存在失败。即使在 COVID-19 控制相对较好的国家,HCW 的感染风险也高于一般人群,医院内暴发会通过在暴发期间隔离大量 HCW 对劳动力能力产生重大影响。即使在社区发病率较低的情况下,医院暴发的发生也突显了医院的高风险环境。该研究结束后,澳大利亚 COVID-19 出现了反弹,发生了多起医院暴发。我们建议对 HCW 感染进行正式报告、对医院内暴发进行检测方案、对员工进行分组以最大程度地减少影响,以及改进个人防护设备指南,为 HCW 提供预防性和最佳保护。