Division of Clinical Pharmacology, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, Ohio, USA.
Clin Pharmacol Ther. 2021 Jun;109(6):1639-1647. doi: 10.1002/cpt.2148. Epub 2021 Jan 7.
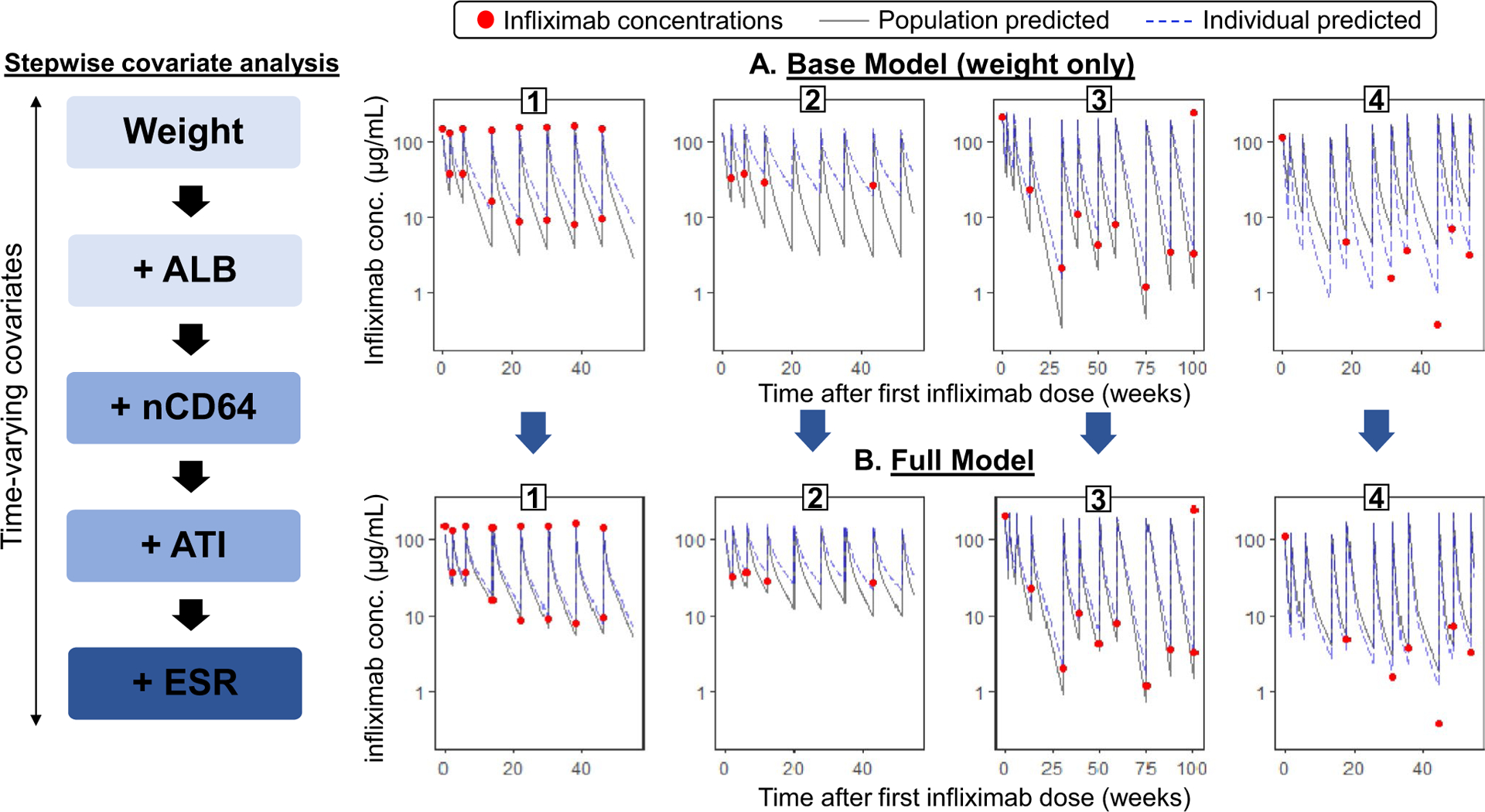
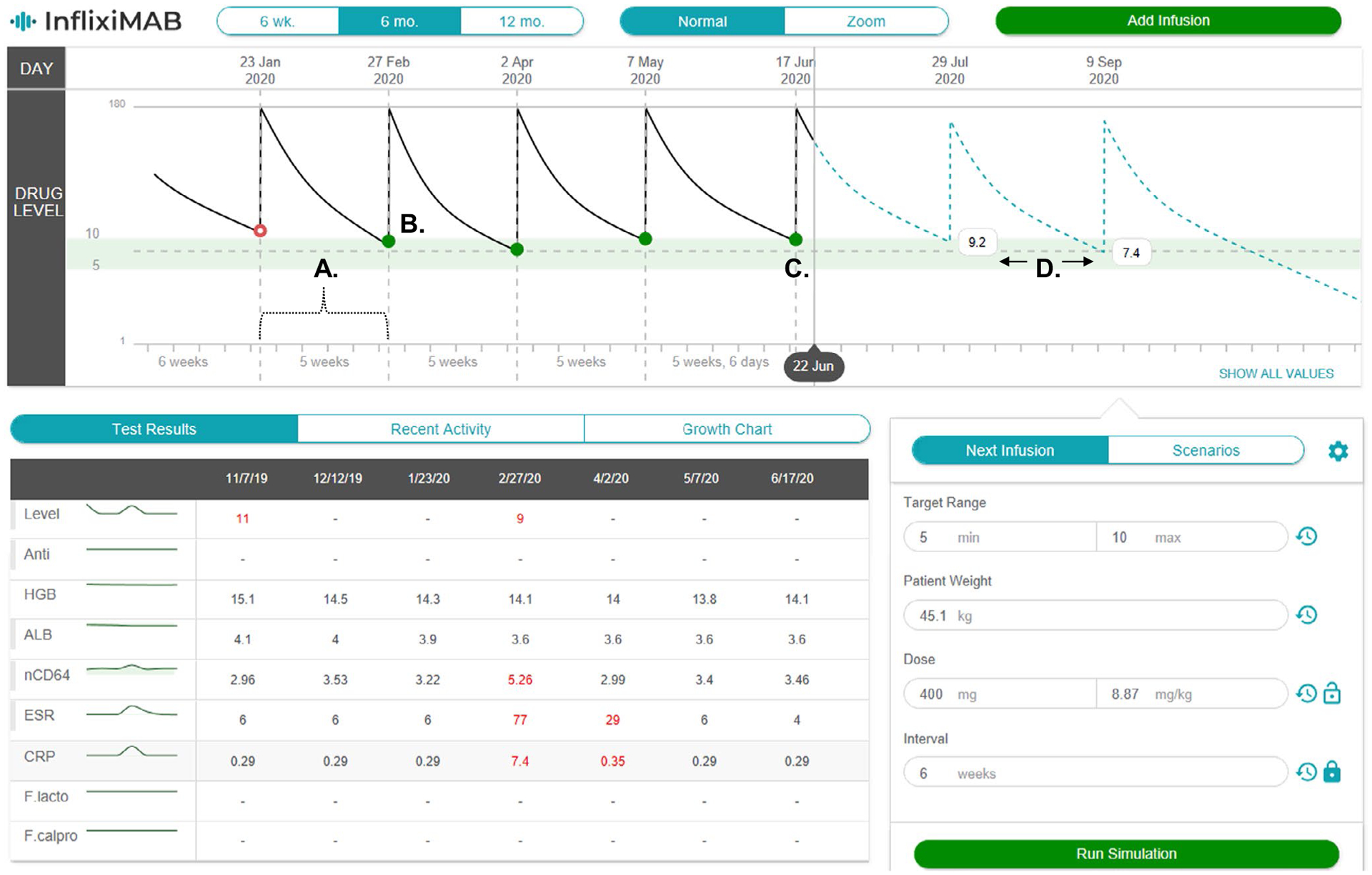
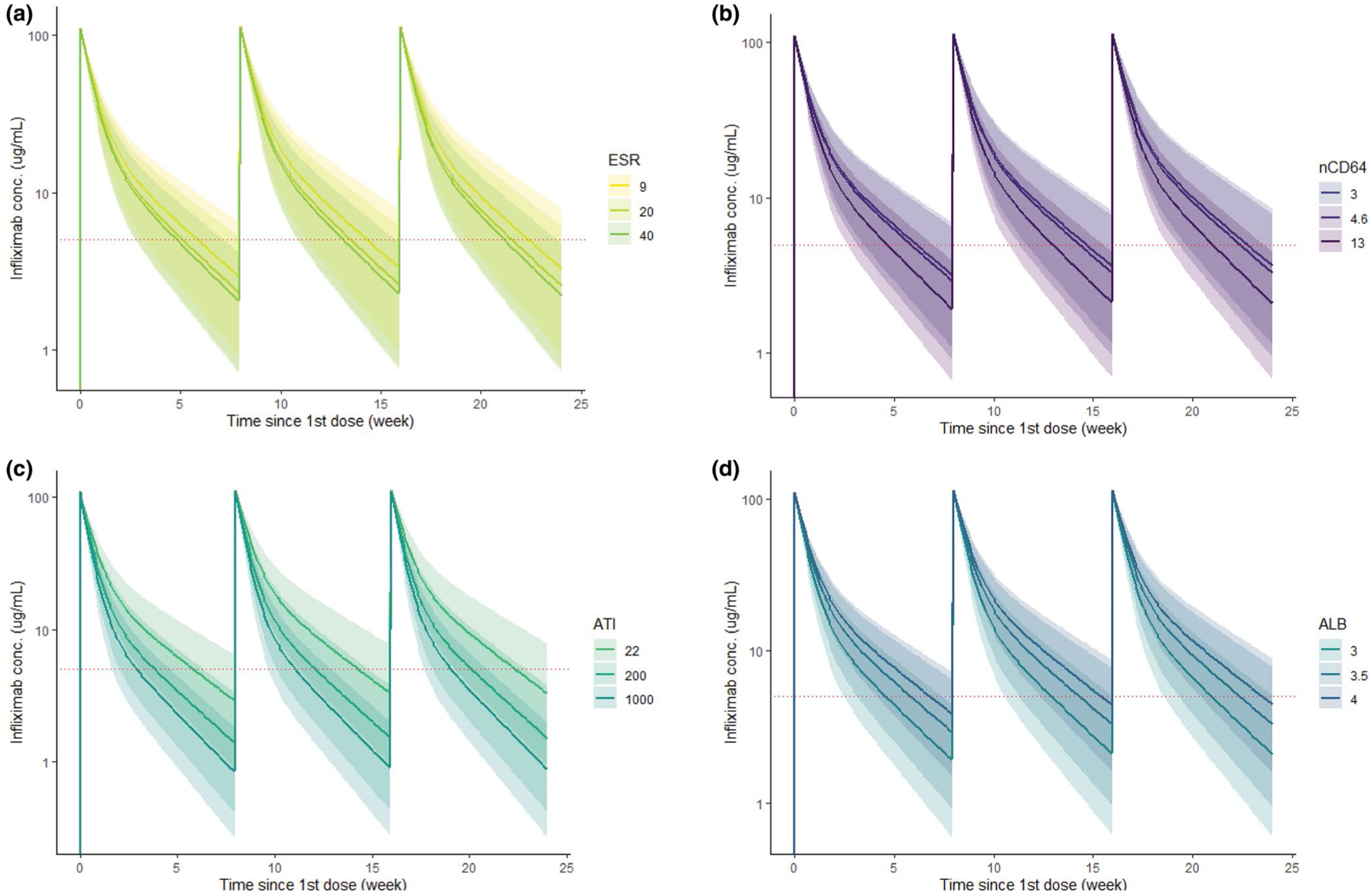
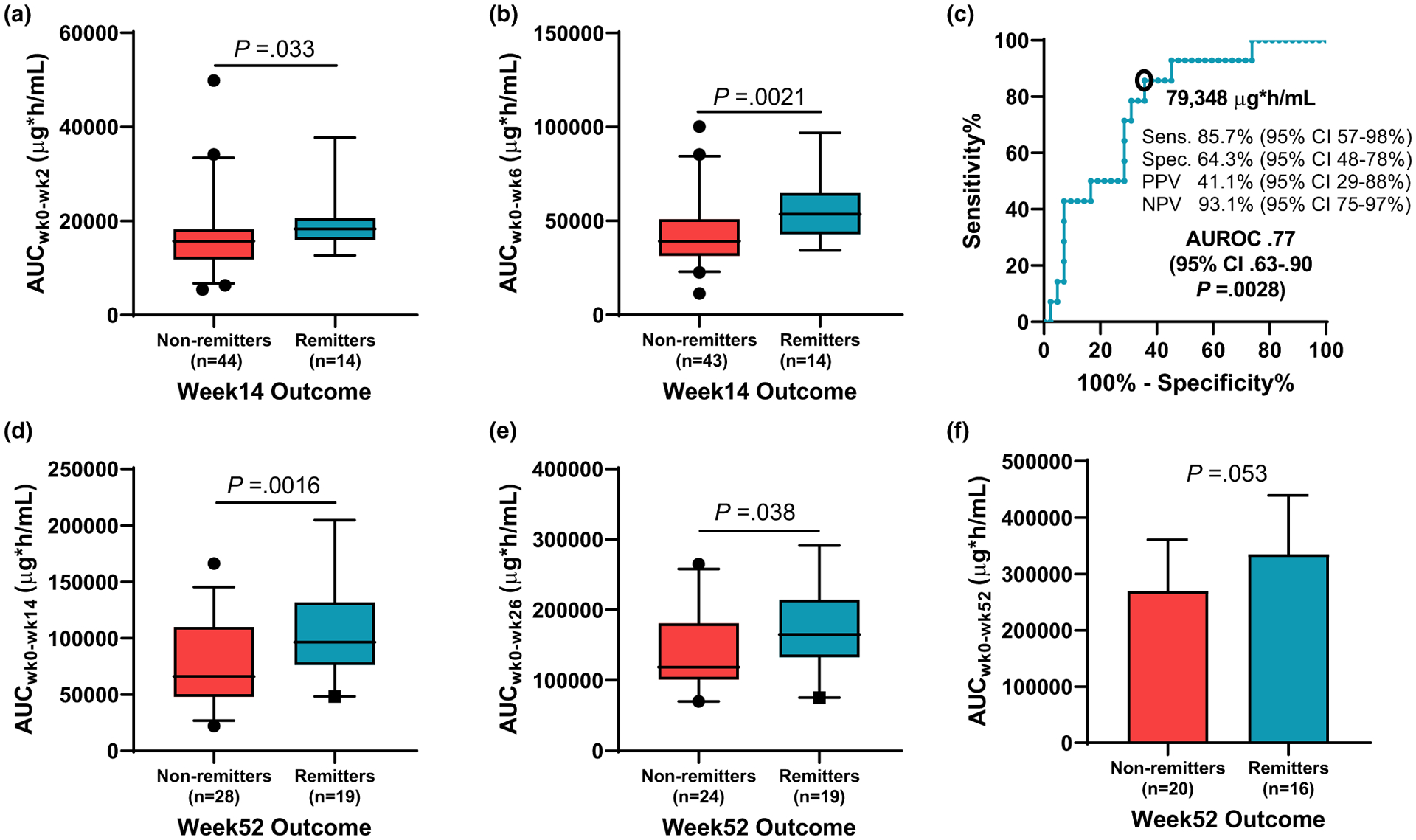
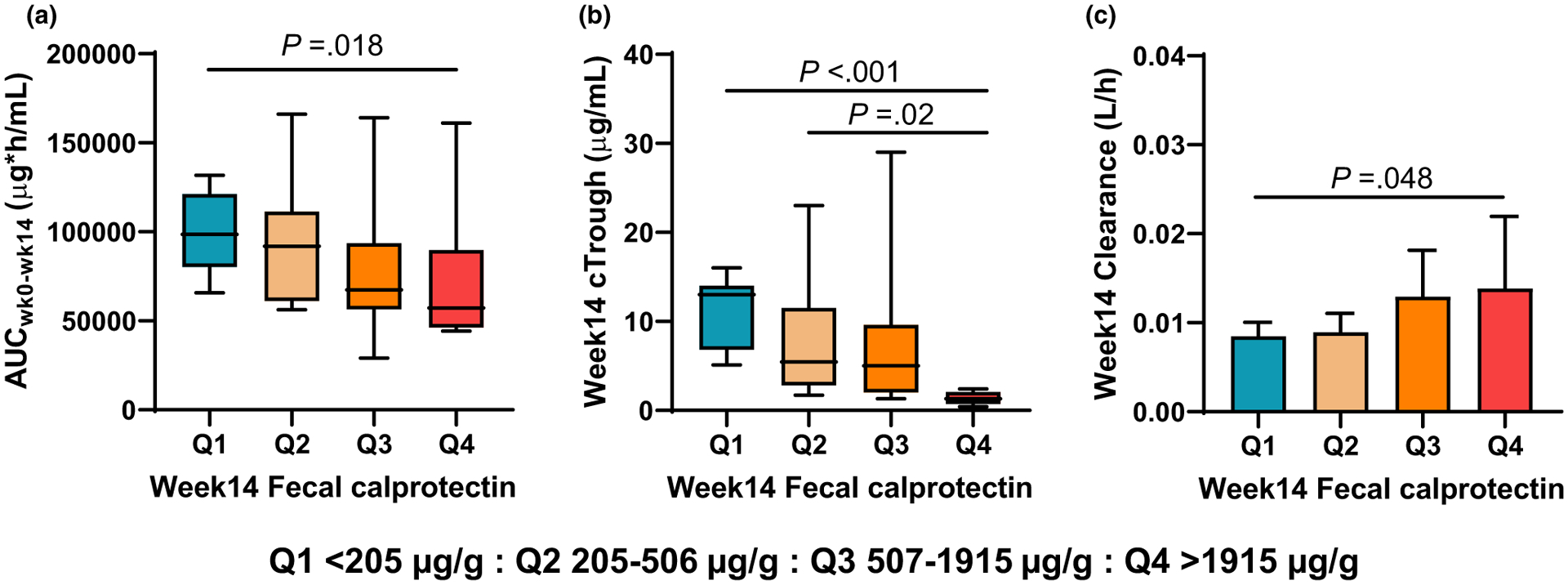
Standard-of-care infliximab dosing regimens were developed prior to the routine use of therapeutic drug monitoring and identification of target concentrations. Not surprisingly, subtherapeutic infliximab concentrations in pediatric Crohn's disease (CD) are common. The primary aim was to conduct a real-world pharmacokinetic (PK) evaluation to discover blood biomarkers of rapid clearance, identify exposure targets, and a secondary aim to translate PK modeling to the clinic. In a multicenter observational study, 671 peak and trough infliximab concentrations from 78 patients with CD were analyzed with a drug-tolerant assay (Esoterix; LabCorp, Calabasas, CA). Individual area under the curve (AUC) estimates were generated as a measure of drug exposure over time. Population PK modeling (nonlinear mixed-effect modeling) identified serum albumin, antibody to infliximab, erythrocyte sedimentation rate (ESR), and neutrophil CD64 as biomarkers for drug clearance. Week 14 and week 52 biochemical remitters (fecal calprotectin < 250 µg/g) had higher infliximab exposure (AUC) throughout induction. The optimal infliximab AUC target during induction for week 14 biochemical remission was 79,348 µg*h/mL (area under the receiver operating characteristic curve (AUROC) 0.77, [0.63-0.90], 85.7% sensitive, and 64.3% specific) with those exceeding the AUC target more likely to achieve a surgery-free week 52 biochemical remission (OR 4.3, [1.2-14.6]). Pretreatment predictors for subtherapeutic week 14 AUC included neutrophil CD64 > 6 (OR 4.5, [1.4-17.8]), ESR > 30 mm/h (OR 3.8, [1.4-11]), age < 10 years old (OR 4.2, [1.2-20]), and weight < 30 kg (OR 6.6, [2.1-25]). We created a decision-support PK dashboard with an iterative process and embedded the modeling program within the electronic health record. Model-informed precision dosing guided by real-world PKs is now available at the bedside in real-time.
标准护理 infliximab 给药方案是在常规使用治疗药物监测和确定目标浓度之前制定的。毫不奇怪,儿科克罗恩病 (CD) 中存在治疗性 infliximab 浓度不足是很常见的。主要目的是进行真实世界的药代动力学 (PK) 评估,以发现快速清除的血液生物标志物,确定暴露目标,次要目的是将 PK 模型转化为临床。在一项多中心观察性研究中,对 78 例 CD 患者的 671 个峰值和谷值 infliximab 浓度进行了分析,采用了一种药物耐受测定法 (Esoterix; LabCorp, Calabasas, CA)。个体 AUC 估计值作为衡量药物随时间暴露的指标。群体 PK 模型 (非线性混合效应模型) 确定了血清白蛋白、抗 infliximab 抗体、红细胞沉降率 (ESR) 和中性粒细胞 CD64 是药物清除的生物标志物。第 14 周和第 52 周生化缓解者 (粪便钙卫蛋白 < 250μg/g) 在诱导期内具有更高的 infliximab 暴露 (AUC)。第 14 周生化缓解的诱导期内最佳 infliximab AUC 目标为 79348μg*h/mL (AUC 接受者操作特征曲线 (AUROC) 0.77 [0.63-0.90],85.7%敏感,64.3%特异),超过 AUC 目标的患者更有可能实现第 52 周无手术的生化缓解 (OR 4.3 [1.2-14.6])。第 14 周 AUC 治疗性不足的预处理预测因子包括中性粒细胞 CD64>6 (OR 4.5 [1.4-17.8])、ESR>30mm/h (OR 3.8 [1.4-11])、年龄 <10 岁 (OR 4.2 [1.2-20]) 和体重 <30kg (OR 6.6 [2.1-25])。我们创建了一个具有迭代过程的决策支持 PK 仪表板,并将建模程序嵌入电子健康记录中。现在,基于真实世界 PK 的模型指导下的精确剂量调整可在床边实时提供。