Division of Endocrinology, Diabetes and Metabolism, University of Florida, Gainesville, FL.
Division of General Internal Medicine, University of Florida, Gainesville, FL.
Diabetes Care. 2021 Feb;44(2):399-406. doi: 10.2337/dc20-1997. Epub 2020 Dec 21.
Assess the prevalence of nonalcoholic fatty liver disease (NAFLD) and of liver fibrosis associated with nonalcoholic steatohepatitis in unselected patients with type 2 diabetes mellitus (T2DM).
A total of 561 patients with T2DM (age: 60 ± 11 years; BMI: 33.4 ± 6.2 kg/m; and HbA: 7.5 ± 1.8%) attending primary care or endocrinology outpatient clinics and unaware of having NAFLD were recruited. At the visit, volunteers were invited to be screened by elastography for steatosis and fibrosis by controlled attenuation parameter (≥274 dB/m) and liver stiffness measurement (LSM; ≥7.0 kPa), respectively. Secondary causes of liver disease were ruled out. Diagnostic panels for prediction of advanced fibrosis, such as AST-to-platelet ratio index (APRI) and Fibrosis-4 (FIB-4) index, were also measured. A liver biopsy was performed if results were suggestive of fibrosis.
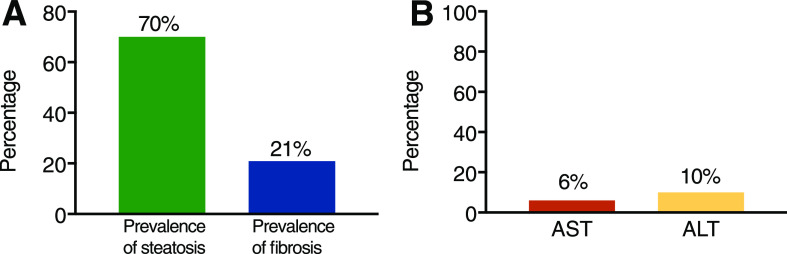
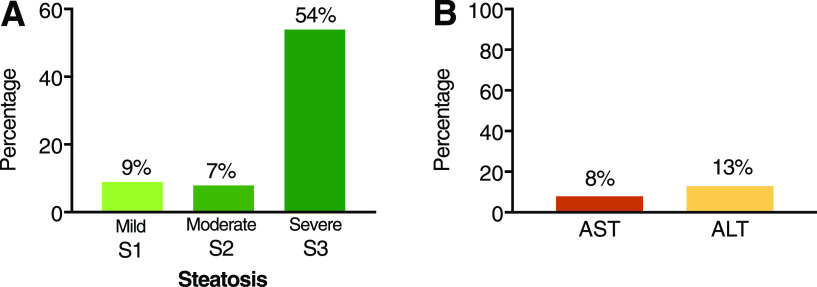
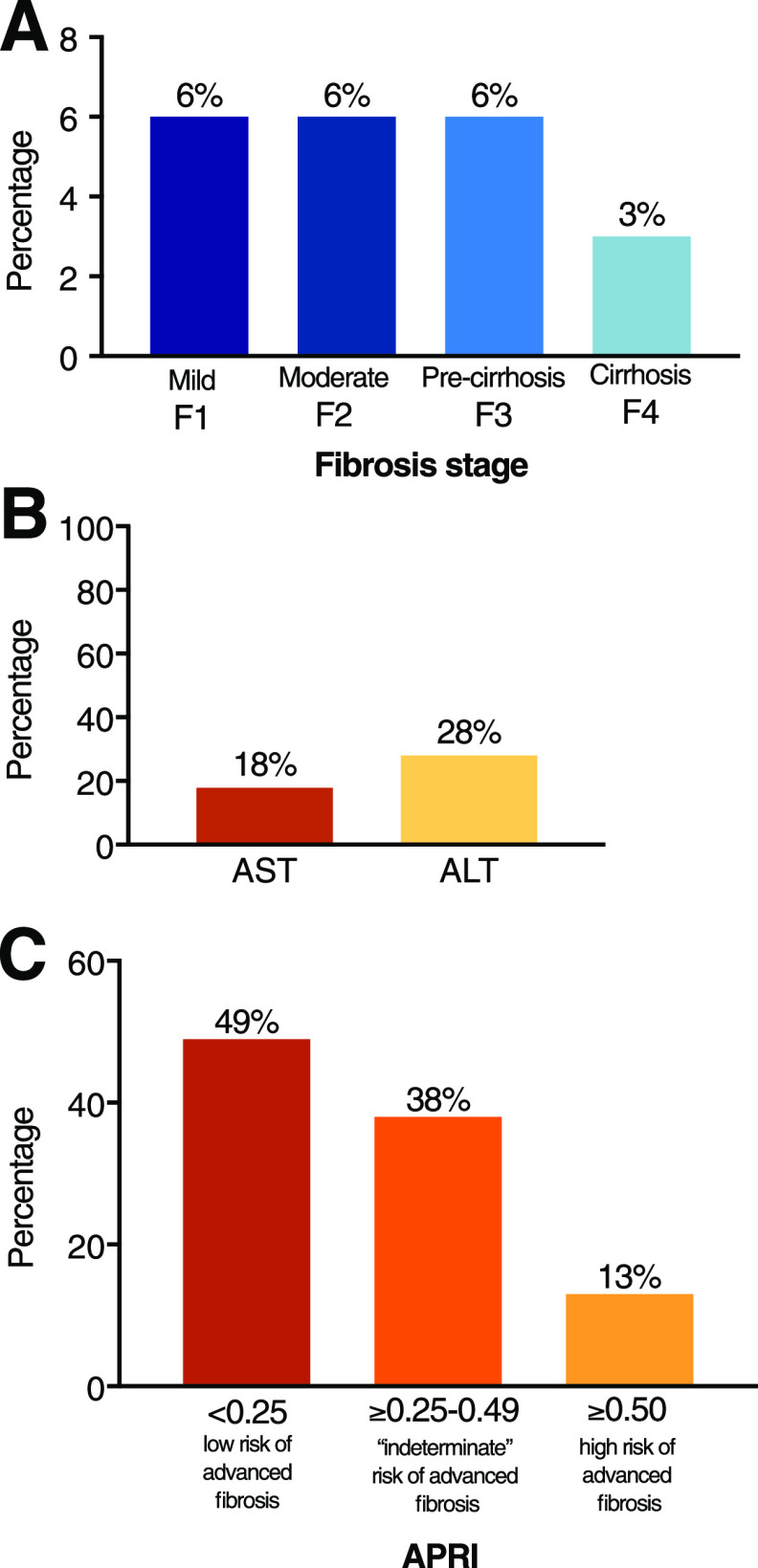
The prevalence of steatosis was 70% and of fibrosis 21% (LSM ≥7.0 kPa). Moderate fibrosis (F2: LSM ≥8.2 kPa) was present in 6% and severe fibrosis or cirrhosis (F3-4: LSM ≥9.7 kPa) in 9%, similar to that estimated by FIB-4 and APRI panels. Noninvasive testing was consistent with liver biopsy results. Elevated AST or ALT ≥40 units/L was present in a minority of patients with steatosis (8% and 13%, respectively) or with liver fibrosis (18% and 28%, respectively). This suggests that AST/ALT alone are insufficient as initial screening. However, performance may be enhanced by imaging (e.g., transient elastography) and plasma diagnostic panels (e.g., FIB-4 and APRI).
Moderate-to-advanced fibrosis (F2 or higher), an established risk factor for cirrhosis and overall mortality, affects at least one out of six (15%) patients with T2DM. These results support the American Diabetes Association guidelines to screen for clinically significant fibrosis in patients with T2DM with steatosis or elevated ALT.
评估非酒精性脂肪性肝病(NAFLD)和非酒精性脂肪性肝炎相关肝纤维化在未经选择的 2 型糖尿病(T2DM)患者中的流行情况。
共招募了 561 名 T2DM 患者(年龄:60 ± 11 岁;BMI:33.4 ± 6.2 kg/m;HbA:7.5 ± 1.8%),他们在初级保健或内分泌科门诊就诊,且不知道自己患有 NAFLD。在就诊时,志愿者被邀请通过瞬时弹性成像进行肝脂肪变和纤维化的筛查,肝脂肪变通过受控衰减参数(≥274 dB/m),纤维化通过肝硬度测量(LSM;≥7.0 kPa)。排除了其他肝脏疾病的继发性病因。还测量了用于预测晚期纤维化的诊断性面板,如天冬氨酸转氨酶-血小板比值指数(APRI)和纤维化-4 指数(FIB-4 指数)。如果结果提示纤维化,则进行肝活检。
肝脂肪变的患病率为 70%,纤维化的患病率为 21%(LSM≥7.0 kPa)。中度纤维化(F2:LSM≥8.2 kPa)的患病率为 6%,严重纤维化或肝硬化(F3-4:LSM≥9.7 kPa)的患病率为 9%,与 FIB-4 和 APRI 面板估计的相似。非侵入性检测与肝活检结果一致。脂肪变患者中仅有少数 AST 或 ALT≥40 单位/L(分别为 8%和 13%),纤维化患者中仅有少数 AST 或 ALT≥40 单位/L(分别为 18%和 28%)。这表明 AST/ALT 单独作为初始筛查并不充分。然而,通过影像学(例如,瞬时弹性成像)和血浆诊断性面板(例如,FIB-4 和 APRI)可以提高其性能。
中重度纤维化(F2 或更高)是肝硬化和总体死亡率的一个既定危险因素,至少影响 1/6(15%)的 T2DM 患者。这些结果支持美国糖尿病协会指南,即对有脂肪变或 ALT 升高的 T2DM 患者进行临床显著纤维化的筛查。