Department of Obstetrics and Gynecology, Penn State Hershey, Hershey, PA, USA.
AbbVie, North Chicago, IL, USA.
Womens Health (Lond). 2020 Jan-Dec;16:1745506520965898. doi: 10.1177/1745506520965898.
Evaluate all-cause and endometriosis-related health care resource utilization and costs among newly diagnosed endometriosis patients with high-risk versus low-risk opioid use or patients with chronic versus non-chronic opioid use.
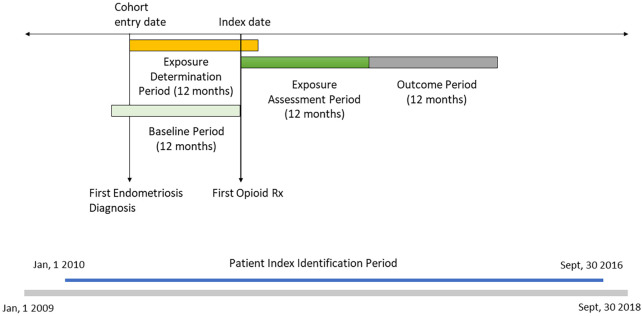
A retrospective analysis of IBM MarketScan Commercial Claims data from 2009 to 2018 was performed for females aged 18 to 49 with newly diagnosed endometriosis (International Classification of Diseases, Ninth Edition code: 617.xx; International Classification of Diseases, Tenth Edition code: N80.xx). Two sub-cohorts were identified: high-risk (⩾1 day with ⩾90 morphine milligram equivalents per day or ⩾1-day concomitant benzodiazepine use) or chronic opioid utilization (⩾90-day supply prescribed or ⩾10 opioid prescriptions). High-risk or chronic utilization was evaluated during the 12-month assessment period after the index date. Index date was the first opioid prescription within 12 months following endometriosis diagnosis. All outcomes were assessed over 12-month post-assessment period while adjusting for demographic and clinical characteristics.
Out of 61,019 patients identified, 18,239 had high-risk opioid use and 5001 chronic opioid use. Health care resource utilization drivers were outpatient visits and pharmacy fills, which were higher among high-risk versus low-risk patients (outpatient visits: 17.49 vs 15.51; pharmacy fills: 19.58 vs 16.88, p < 0.0001). Chronic opioid users had a higher number of outpatient visits (19.53 vs 15.00, p < 0.0001) and pharmacy fills (23.18 vs 16.43, p < 0.0001) compared to non-chronic opioid users. High-risk opioid users had significantly higher all-cause health care costs compared to low-risk opioid users (US$16,377 vs US$13,153; p < 0.0001). Chronic opioid users also had significantly higher all-cause health care costs compared to non-chronic opioid users (US$20,930 vs US$12,272; p < 0.0001). Similar patterns were observed among endometriosis-related HCRU, except pharmacy fills among high-risk and chronic sub-cohorts.
This analysis demonstrates significantly higher all-cause and endometriosis-related health care resource utilization and total costs for high-risk opioid users compared to low-risk opioid users among newly diagnosed endometriosis patients over 1 year. Similar trends were observed for comparing chronic opioid users with non-chronic opioid users, except for endometriosis-related pharmacy fills and associated costs.
评估新诊断为子宫内膜异位症的患者中,高风险与低风险阿片类药物使用者或慢性与非慢性阿片类药物使用者的全因和与子宫内膜异位症相关的医疗资源利用和成本。
对 2009 年至 2018 年 IBM MarketScan 商业索赔数据进行了回顾性分析,纳入年龄在 18 至 49 岁、新诊断为子宫内膜异位症(国际疾病分类第 9 版代码:617.xx;国际疾病分类第 10 版代码:N80.xx)的女性患者。确定了两个亚组:高风险(每天使用 ⩾1 天且每天使用 ⩾90 毫克吗啡等效物或每天同时使用 ⩾1 天苯二氮䓬类药物)或慢性阿片类药物使用(开具 ⩾90 天的处方或 ⩾10 次阿片类药物处方)。在索引日期后的 12 个月评估期内评估高风险或慢性使用情况。索引日期为子宫内膜异位症诊断后 12 个月内首次开具阿片类药物处方的日期。所有结果在调整人口统计学和临床特征后,在 12 个月的评估后期间进行评估。
在确定的 61019 例患者中,有 18239 例为高风险阿片类药物使用者,5001 例为慢性阿片类药物使用者。门诊就诊和药房配药是医疗资源利用的驱动因素,高风险患者的门诊就诊和药房配药次数均高于低风险患者(门诊就诊:17.49 次比 15.51 次;药房配药:19.58 次比 16.88 次,均 P<0.0001)。慢性阿片类药物使用者的门诊就诊次数(19.53 次比 15 次,P<0.0001)和药房配药次数(23.18 次比 16.43 次,P<0.0001)均高于非慢性阿片类药物使用者。与低风险阿片类药物使用者相比,高风险阿片类药物使用者的全因医疗费用显著更高(16377 美元比 13153 美元;P<0.0001)。与非慢性阿片类药物使用者相比,慢性阿片类药物使用者的全因医疗费用也显著更高(20930 美元比 12272 美元;P<0.0001)。在与子宫内膜异位症相关的 HCRU 中也观察到了类似的模式,除了高风险和慢性亚组的药房配药次数外。
这项分析表明,在新诊断为子宫内膜异位症的患者中,与低风险阿片类药物使用者相比,高风险阿片类药物使用者在 1 年内的全因和与子宫内膜异位症相关的医疗资源利用和总成本显著更高。对于比较慢性阿片类药物使用者与非慢性阿片类药物使用者,也观察到了类似的趋势,除了与子宫内膜异位症相关的药房配药次数和相关成本外。