Li Ming, Yue Jinbo, Wan Xiangbo, Hua Bin, Yang Qiuan, Yang Pei, Zhang Zijian, Pei Qian, Han Weidong, Xu Yaping, Xia Xuefeng
Department of Radiation Oncology, Beijing Hospital/National Center of Gerontology, Beijing, China.
Department of Radiation Oncology, Shandong Cancer Hospital Affiliated to Shandong University/Shandong Academy of Medical Sciences, Jinan, China.
Front Oncol. 2020 Dec 11;10:588859. doi: 10.3389/fonc.2020.588859. eCollection 2020.
The aim of this study was to develop a widely accepted prognostic nomogram and establish a risk-adapted PMRT strategy based on locoregional recurrence for pT1-2N1M0 breast cancer.
A total of 3,033 patients with pT1-2N1M0 breast cancer treated at 6 participating institutions between 2000 and 2016 were retrospectively reviewed. A nomogram was developed to predicted locoregional recurrence-free survival (LRFS). A propensity score-matched (PSM) analyses was performed in risk-adapted model.
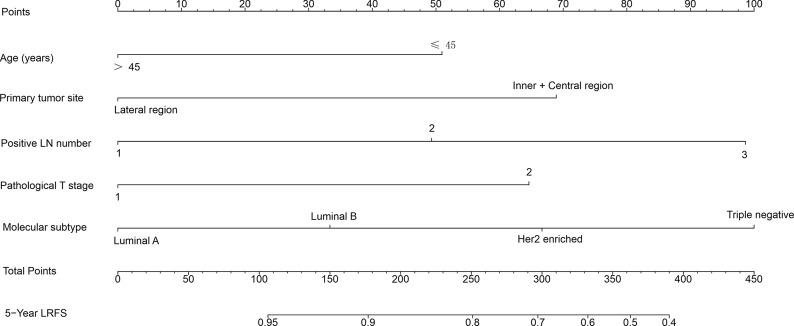
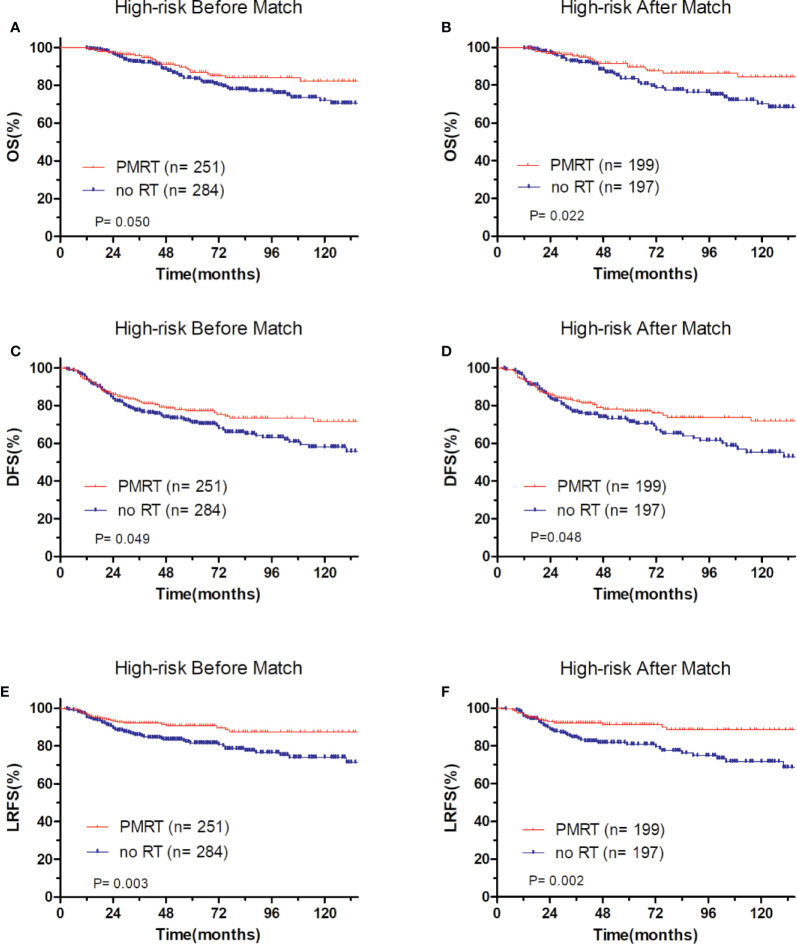
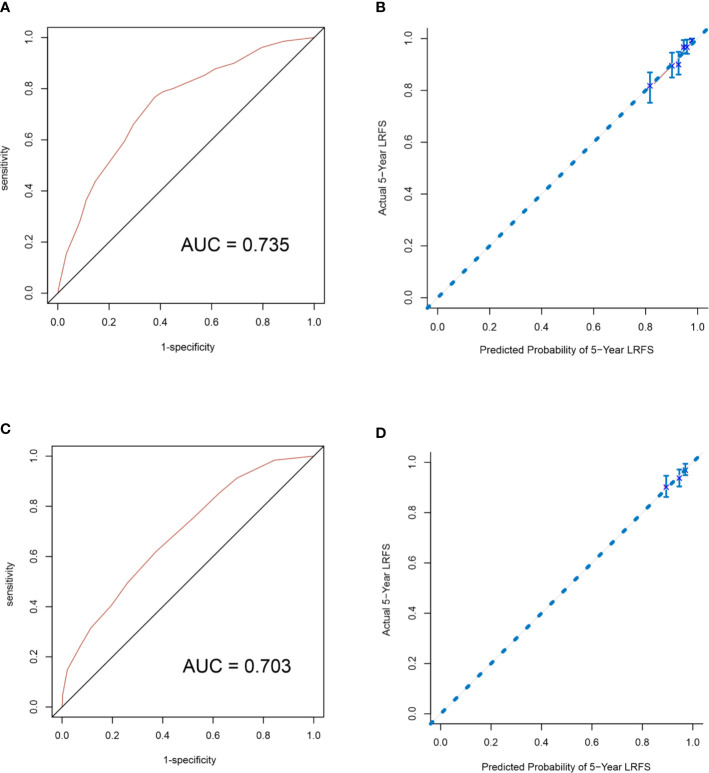
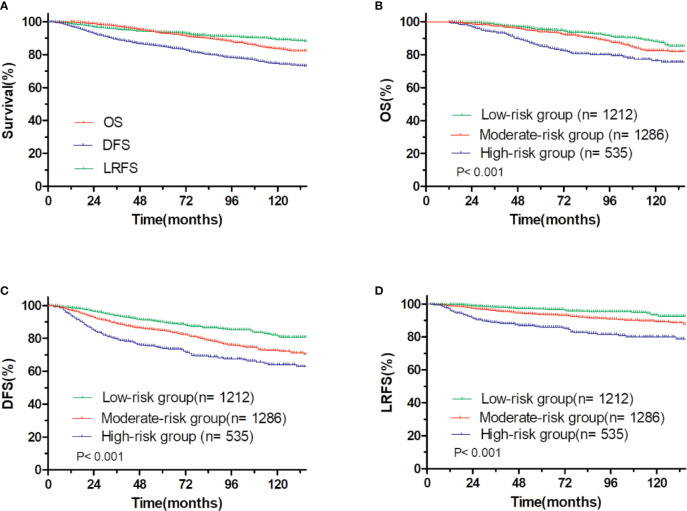
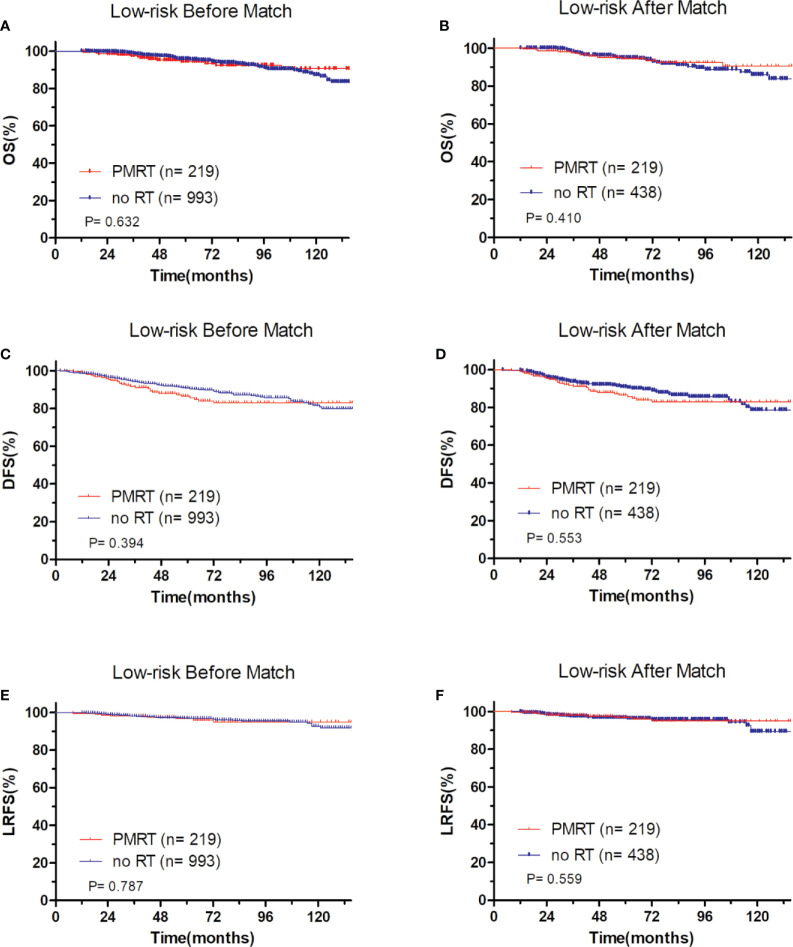
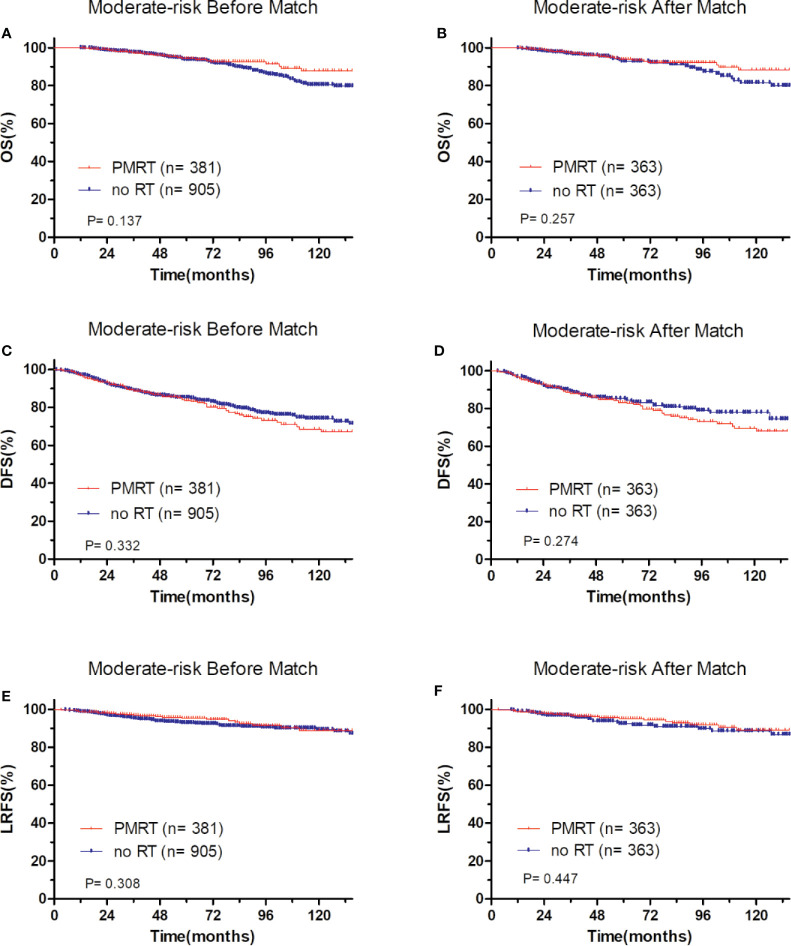
With the median follow-up of 65.0 months, the 5-year overall survival (OS), disease free survival (DFS) and LRFS were 93.0, 84.8, and 93.6%, respectively. There was no significant difference between patients who received PMRT or not for the entire group. A nomogram was developed and validated to estimate the probability of 5-year LRFS based on five independent factors including age, primary tumor site, positive lymph nodes number, pathological T stage, and molecular subtype that were selected by a multivariate analysis of patients who did not receive PMRT in the primary cohort. According to the total nomogram risk scores, the entire patients were classified into low- (40.0%), moderate- (42.4%), and high-risk group (17.6%). The 5-year outcomes were significantly different among these three groups (P<0.001). In low-risk group, patients who received PMRT or not both achieved a favorable OS, DFS, and LRFS. In moderate-risk group, no differences in OS, DFS, and LRFS were observed between PMRT and no PMRT patients. In high-risk group, compared with no PMRT, PMRT resulted in significantly different OS (86.8 vs 83.9%, P = 0.050), DFS (77.2 vs 70.9%, P = 0.049), and LRFS (90.8 vs. 81.6%, P = 0.003). After PSM adjustment, there were no significant differences in OS, DFS, and LRFS in low-risk and moderate-risk groups. However, in the high-risk group, PMRT still resulted in significantly better OS, DFS and improved LRFS.
The proposed nomogram provides an individualized risk estimate of LRFS in patients with pT1-2N1M0 breast cancer. Risk-adapted PMRT for high-risk patients is a viable effective strategy.
本研究旨在开发一种广泛接受的预后列线图,并基于局部区域复发情况为pT1-2N1M0乳腺癌建立一种风险适应性的术后放疗(PMRT)策略。
回顾性分析了2000年至2016年间在6家参与机构接受治疗的3033例pT1-2N1M0乳腺癌患者。开发了一种列线图来预测无局部区域复发生存期(LRFS)。在风险适应性模型中进行了倾向评分匹配(PSM)分析。
中位随访时间为65.0个月,5年总生存率(OS)、无病生存率(DFS)和LRFS分别为93.0%、84.8%和93.6%。整个组中接受或未接受PMRT的患者之间无显著差异。基于多因素分析从原发队列中未接受PMRT的患者中选择的年龄、原发肿瘤部位、阳性淋巴结数量、病理T分期和分子亚型这五个独立因素,开发并验证了一种列线图以估计5年LRFS的概率。根据列线图总风险评分,将所有患者分为低风险组(40.0%)、中风险组(42.4%)和高风险组(17.6%)。这三组的5年结局有显著差异(P<0.001)。在低风险组中,接受或未接受PMRT的患者均获得了良好的OS、DFS和LRFS。在中风险组中,接受PMRT和未接受PMRT的患者在OS、DFS和LRFS方面未观察到差异。在高风险组中,与未接受PMRT相比,PMRT导致OS(86.8%对83.9%,P = 0.050)、DFS(77.2%对70.9%,P = 0.049)和LRFS(90.8%对81.6%,P = 0.003)有显著差异。经过PSM调整后,低风险和中风险组在OS, DFS和LRFS方面无显著差异。然而,在高风险组中,PMRT仍然导致显著更好的OS、DFS和改善的LRFS。
所提出的列线图为pT1-2N1M0乳腺癌患者提供了LRFS的个体化风险估计。对高风险患者采用风险适应性PMRT是一种可行的有效策略。