Department of Radiation Oncology, The Fourth Hospital of Hebei Medical University, Shijiazhuang, 050035, China.
Radiat Oncol. 2024 Sep 13;19(1):120. doi: 10.1186/s13014-024-02510-w.
To explore the high-risk factors affecting the prognosis of pTNM patients after mastectomy, establish a nomogram prediction model, and screen the radiotherapy benefit population.
The clinical data of 936 patients with pTNM who underwent mastectomy in the fourth hospital of Hebei Medical University from 2010 to 2016 were retrospectively analyzed. There were 583 patients received postmastectomy radiotherapy(PMRT), and 325 patients without PMRT. Group imbalances were mitigated using the propensity score matching (PSM) method, and the log-rank test was employed to compare overall survival (OS) and disease-free survival (DFS) between the cohorts. The efficacy of PMRT across various risk groups was evaluated using a nomogram model.
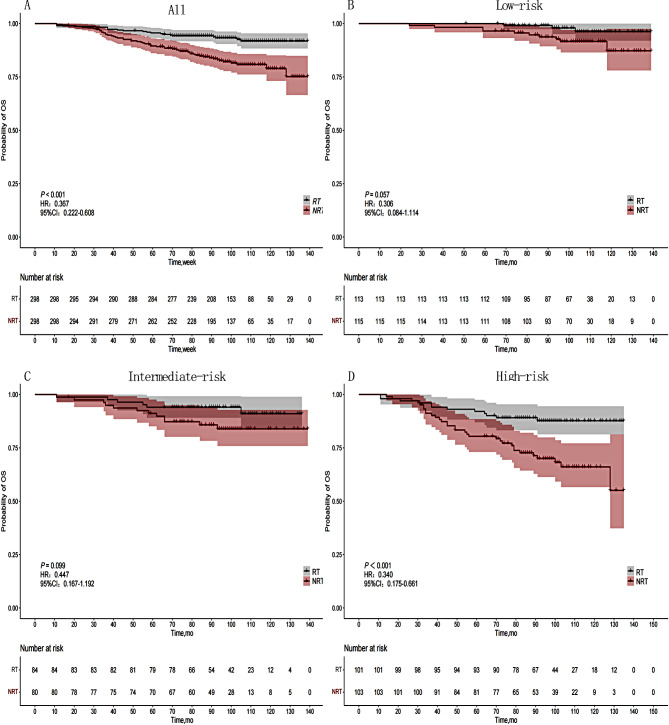
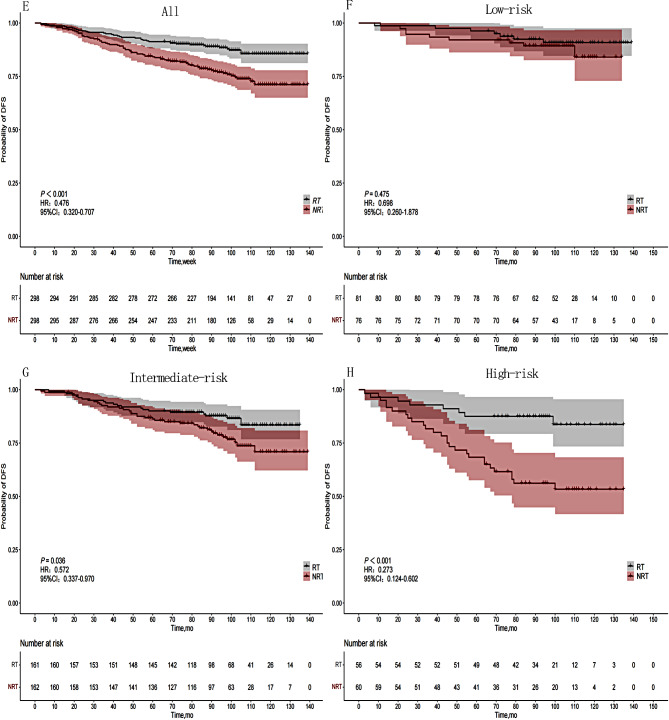
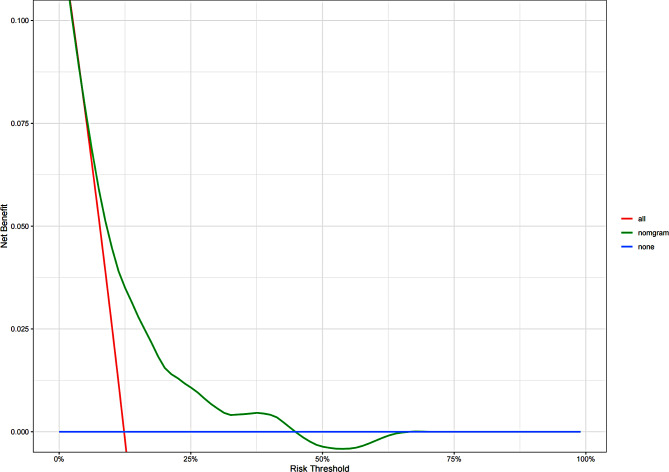
The median follow-up period was 98 months, Patients who received PMRT demonstrated significantly improved 5-year and 8-year OS and DFS compared to those who did not (P < 0.001). Multivariate analysis revealed that age, primary tumor site, positive lymph node, stage, and Ki-67 level independently influenced OS, while age, primary tumor site, and stage independently affected DFS. PMRT drastically enhanced OS in the high-risk group (P = 0.001), but did not confer benefits in the low-risk and intermediate risk groups (P = 0.057, P = 0.099). PMRT led to a significant improvement in disease-free survival (DFS) among patients in the intermediate and high-risk groups (P = 0.036, P = 0.001), whereas the low-risk group did not experience a significant benefit (P = 0.475).
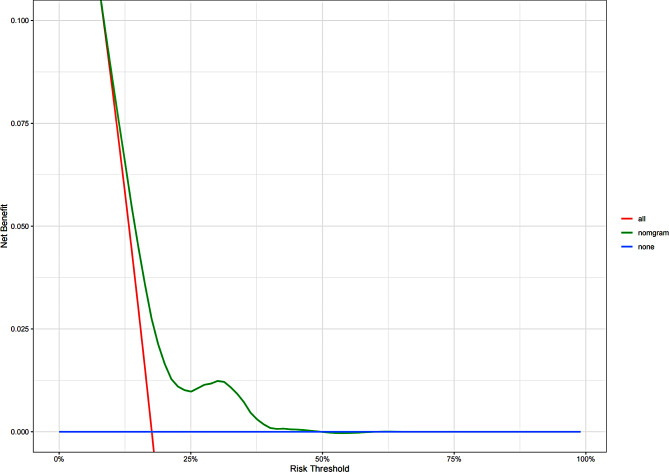
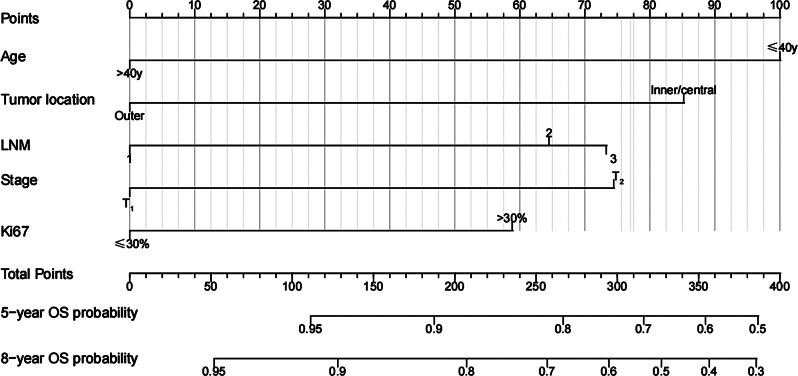
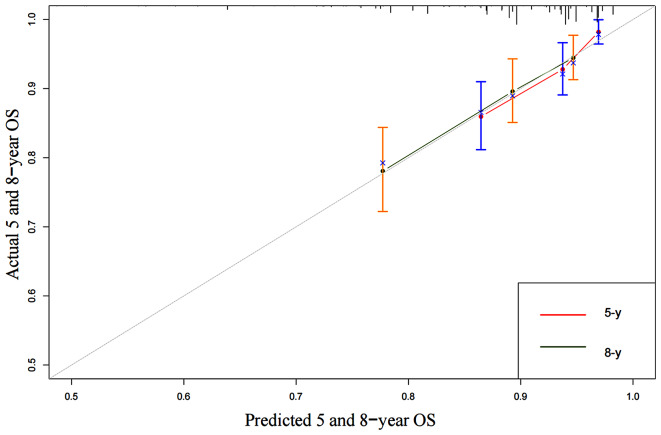
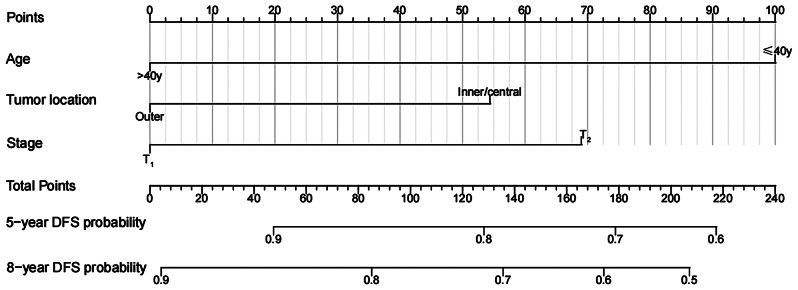
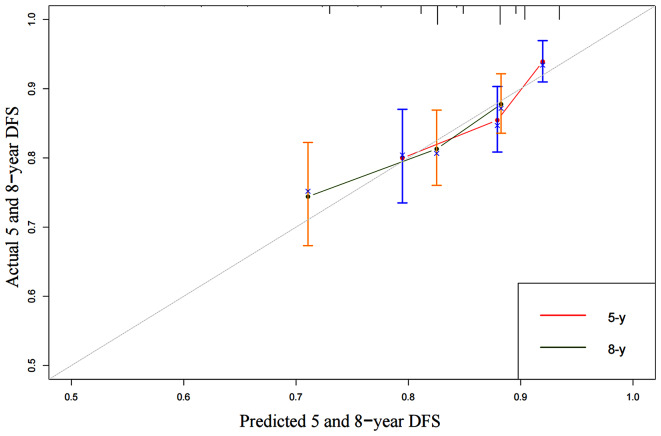
Age ≤ 40 years, tumor located in the inner quadrant or central area, T stage, 2-3 lymph nodes metastasis, and Ki67 > 30% were the high-risk factors affecting the prognosis of this cohort of patients. In OS nomogram, patients with a risk score of 149 or higher who received PMRT exhibited improved OS. Similarly, in DFS nomogram, patients with a risk score of 123 or higher who received PMRT demonstrated enhanced DFS.
探讨影响乳腺癌改良根治术后 pTNM 患者预后的高危因素,建立列线图预测模型,并筛选放疗获益人群。
回顾性分析 2010 年至 2016 年河北医科大学第四医院收治的 936 例 pTNM 乳腺癌改良根治术后患者的临床资料,其中 583 例患者接受了术后放疗(PMRT),325 例患者未接受 PMRT。采用倾向评分匹配(PSM)方法减轻组间不平衡,采用 log-rank 检验比较两组患者的总生存(OS)和无病生存(DFS)。通过列线图模型评估 PMRT 在不同风险组中的疗效。
中位随访时间为 98 个月,接受 PMRT 的患者 5 年和 8 年 OS 和 DFS 明显优于未接受 PMRT 的患者(P<0.001)。多因素分析显示,年龄、原发肿瘤部位、阳性淋巴结、分期和 Ki-67 水平独立影响 OS,而年龄、原发肿瘤部位和分期独立影响 DFS。PMRT 显著提高了高危组的 OS(P=0.001),但在低危和中危组中没有获益(P=0.057,P=0.099)。PMRT 显著改善了中危和高危组患者的无病生存(DFS)(P=0.036,P=0.001),而低危组患者未获得显著获益(P=0.475)。
年龄≤40 岁、肿瘤位于内象限或中央区、T 分期、2-3 个淋巴结转移和 Ki67>30%是影响该队列患者预后的高危因素。在 OS 列线图中,风险评分≥149 分且接受 PMRT 的患者 OS 得到改善。同样,在 DFS 列线图中,风险评分≥123 分且接受 PMRT 的患者 DFS 得到提高。