Triplett James D, Shelly Shahar, Livne Guy, Milone Margherita, Kassardjian Charles D, Liewluck Teerin, Kelly Cecilia, Naddaf Elie, Laughlin Ruple S, Lamb Christopher J, Rubin Devon, Dimberg Elliot L, Dubey Divanshu, Mills John R, Mandrekar Jay, Klein Christopher J
Department of Neurology, Mayo Clinic, Rochester, MN, USA.
Guylivne.com, Boston, MA, USA.
Brain Commun. 2020 Dec 13;2(2):fcaa191. doi: 10.1093/braincomms/fcaa191. eCollection 2020.
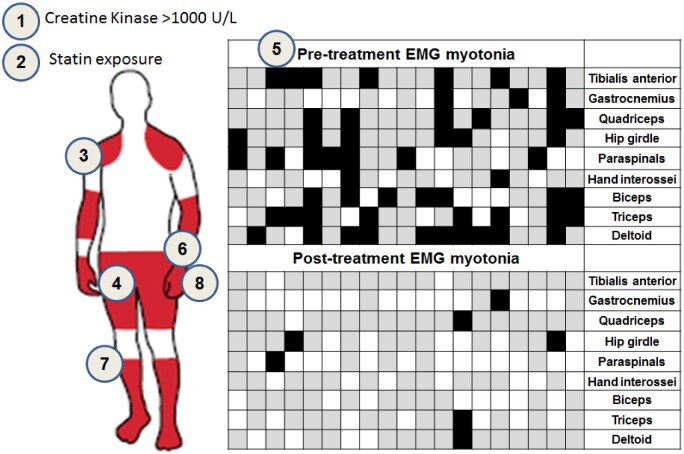
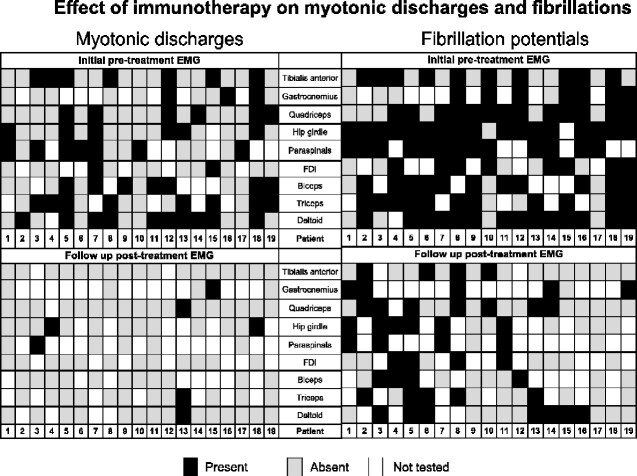
Delayed diagnosis of immunemediated necrotizing myopathy leads to increased morbidity. Patients with the chronic course without 3-hydroxy-3-methylglutaryl-coenzyme-A reductase-IgG or signal recognition particle-IgG are often challenging to diagnose. Immunotherapy response can also be difficult to assess. We created a statistical model to assist immunemediated necrotizing myopathy diagnosis. Electrical myotonia versus fibrillations were reviewed as biomarkers for immunotherapy treatment response. Identified were 119 immunemediated necrotizing myopathy cases and 938 other myopathy patients. Inclusion criteria included all having electrophysiological evaluations, muscle biopsies showing inflammatory/necrotizing myopathies, comprehensively recorded neurological examinations, and creatine kinase values. Electrical myotonia was recorded in 56% (67/119) of retrospective and 67% (20/30) of our validation immunemediated necrotizing myopathy cohorts, and significantly ( < 0.001) favoured immunemediated necrotizing myopathy over other myopathies: sporadic inclusion body myositis (odds ratio = 4.78); dermatomyositis (odds ratio = 10.61); non-specific inflammatory myopathies (odds ratio = 8.46); limb-girdle muscular dystrophies (odds ratio = 5.34) or mitochondrial myopathies (odds ratio = 14.17). Electrical myotonia occurred in immunemediated necrotizing myopathy seropositive (3-hydroxy-3-methylglutaryl-coenzyme-A reductase-IgG 70%, 37/53; signal recognition particle-IgG 29%, 5/17) and seronegative (51%, 25/49). Multivariate regression analysis of 20 variables identified 8 (including electrical myotonia) in combination accurately predicted immunemediated necrotizing myopathy (97.1% area-under-curve). The model was validated in a separate cohort of 30 immunemediated necrotizing myopathy cases. Delayed diagnosis of cases with electrical myotonia occurred in 24% (16/67, mean 8 months; range 0-194). Half (8/19) had a chronic course and were seronegative, with high model prediction (>86%) at the first visit. Inherited myopathies were commonly first suspected in them. Follow-up evaluation in patients with electrical myotonia on immunotherapy was available in 19 (median 21 months, range 2-124) which reduced from 36% (58/162) of muscles to 7% (8/121; < 0.001). Reduced myotonia correlated with immunotherapy response in 64% (9/14) as well as with median creatine kinase reduction of 1779 U/l (range 401-9238, < 0.001). Modelling clinical features with electrical myotonia is especially helpful in immunemediated necrotizing myopathy diagnostic suspicion among chronic indolent and seronegative cases. Electrical myotonia favours immunemediated necrotizing myopathy diagnosis and can serve as an adjuvant immunotherapy biomarker.
免疫介导性坏死性肌病的延迟诊断会导致发病率增加。对于那些病程呈慢性且不存在3-羟基-3-甲基戊二酰辅酶A还原酶-IgG或信号识别颗粒-IgG的患者,诊断往往具有挑战性。免疫治疗反应也可能难以评估。我们创建了一个统计模型来辅助免疫介导性坏死性肌病的诊断。将电强直与纤颤作为免疫治疗反应的生物标志物进行了评估。共纳入119例免疫介导性坏死性肌病病例和938例其他肌病患者。纳入标准包括均进行了电生理评估、肌肉活检显示为炎症性/坏死性肌病、全面记录的神经系统检查以及肌酸激酶值。在回顾性研究的免疫介导性坏死性肌病队列中,56%(67/119)记录到电强直,在我们的验证性免疫介导性坏死性肌病队列中这一比例为67%(20/30),并且电强直显著(<0.001)支持免疫介导性坏死性肌病的诊断,相对于其他肌病:散发性包涵体肌炎(比值比=4.78);皮肌炎(比值比=10.61);非特异性炎症性肌病(比值比=8.46);肢带型肌营养不良症(比值比=5.34)或线粒体肌病(比值比=14.17)。电强直在免疫介导性坏死性肌病血清阳性(3-羟基-3-甲基戊二酰辅酶A还原酶-IgG 70%,37/53;信号识别颗粒-IgG 29%,5/17)和血清阴性(51%,25/49)患者中均有出现。对20个变量进行多因素回归分析,确定了8个变量(包括电强直)联合起来能够准确预测免疫介导性坏死性肌病(曲线下面积为97.1%)。该模型在另一组30例免疫介导性坏死性肌病病例中得到验证。电强直患者中延迟诊断的病例占24%(16/67,平均8个月;范围0 - 194个月)。其中一半(8/19)病程呈慢性且血清阴性,首次就诊时模型预测值较高(>86%)。这些患者最初常被怀疑患有遗传性肌病。对接受免疫治疗的电强直患者进行随访评估的有19例(中位时间21个月,范围2 - 124个月),肌肉受累比例从36%(58/162)降至7%(8/121;<0.001)。64%(9/14)的患者电强直减轻与免疫治疗反应相关,同时肌酸激酶中位数降低1779 U/l(范围401 - 9238,<0.001)。在慢性隐匿性和血清阴性病例中,利用电强直对临床特征进行建模对于免疫介导性坏死性肌病的诊断怀疑特别有帮助。电强直有助于免疫介导性坏死性肌病的诊断,可作为免疫治疗的辅助生物标志物。