Magnani Christopher J, Bievre Nicolas, Baker Laurence C, Brooks James D, Blayney Douglas W, Hernandez-Boussard Tina
School of Medicine, Stanford University, Stanford, CA, USA.
Department of Statistics, Stanford University, Stanford, CA, USA.
Eur Urol Open Sci. 2021 Jan;23:20-29. doi: 10.1016/j.euros.2020.11.004. Epub 2020 Dec 10.
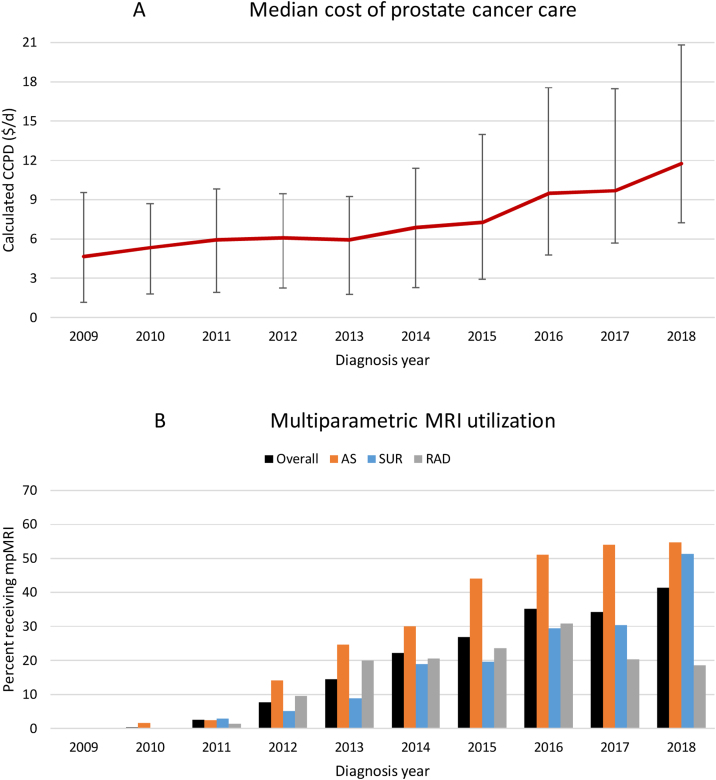
Prostate cancer is the most common cancer in men and second leading cause of cancer-related deaths. Changes in screening guidelines, adoption of active surveillance (AS), and implementation of high-cost technologies have changed treatment costs. Traditional cost-effectiveness studies rely on clinical trial protocols unlikely to capture actual practice behavior, and existing studies use data predating new technologies. Real-world evidence reflecting these changes is lacking.
To assess real-world costs of first-line prostate cancer management.
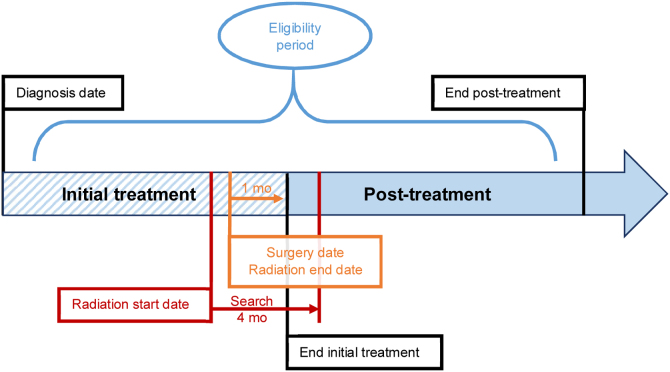
We used clinical electronic health records for 2008-2018 linked with the California Cancer Registry and the Medicare Fee Schedule to assess costs over 24 or 60 mo following diagnosis. We identified surgery or radiation treatments with structured methods, while we used both structured data and natural language processing to identify AS.
Our results are risk-stratified calculated cost per day (CCPD) for first-line management, which are independent of treatment duration. We used the Kruskal-Wallis test to compare unadjusted CCPD while analysis of covariance log-linear models adjusted estimates for age and Charlson comorbidity.
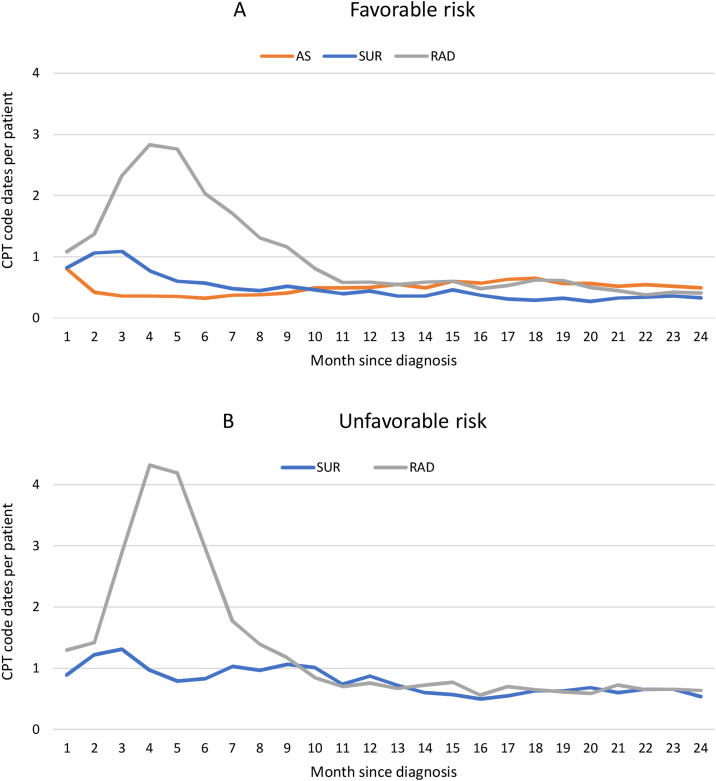
In 3433 patients, surgery (54.6%) was more common than radiation (22.3%) or AS (23.0%). Two years following diagnosis, AS ($2.97/d) was cheaper than surgery ($5.67/d) or radiation ($9.34/d) in favorable disease, while surgery ($7.17/d) was cheaper than radiation ($16.34/d) for unfavorable disease. At 5 yr, AS ($2.71/d) remained slightly cheaper than surgery ($2.87/d) and radiation ($4.36/d) in favorable disease, while for unfavorable disease surgery ($4.15/d) remained cheaper than radiation ($10.32/d). Study limitations include information derived from a single healthcare system and costs based on benchmark Medicare estimates rather than actual payment exchanges.
Active surveillance was cheaper than surgery (-47.6%) and radiation (-68.2%) at 2 yr for favorable-risk disease, which decreased by 5 yr (-5.6% and -37.8%, respectively). Surgery was less costly than radiation for unfavorable risk for both intervals (-56.1% and -59.8%, respectively).
前列腺癌是男性中最常见的癌症,也是癌症相关死亡的第二大主要原因。筛查指南的变化、主动监测(AS)的采用以及高成本技术的应用改变了治疗成本。传统的成本效益研究依赖于不太可能反映实际临床行为的临床试验方案,并且现有研究使用的是新技术出现之前的数据。缺乏反映这些变化的真实世界证据。
评估一线前列腺癌治疗的真实世界成本。
设计、背景与参与者:我们使用了2008 - 2018年的临床电子健康记录,并与加利福尼亚癌症登记处和医疗保险费用明细表相链接,以评估诊断后24个月或60个月内的成本。我们采用结构化方法识别手术或放射治疗,同时使用结构化数据和自然语言处理来识别主动监测。
我们的结果是按风险分层计算的一线治疗每日成本(CCPD),其与治疗持续时间无关。我们使用Kruskal - Wallis检验比较未调整的CCPD,同时使用协方差对数线性模型分析对年龄和查尔森合并症进行调整后的估计值。
在3433例患者中,手术(54.6%)比放射治疗(22.3%)或主动监测(23.0%)更常见。诊断后两年,在低风险疾病中,主动监测(2.97美元/天)比手术(5.67美元/天)或放射治疗(9.34美元/天)成本更低,而在高风险疾病中,手术(7.17美元/天)比放射治疗(16.34美元/天)成本更低。在5年时,在低风险疾病中,主动监测(2.71美元/天)仍略低于手术(2.87美元/天)和放射治疗(4.36美元/天),而在高风险疾病中,手术(4.15美元/天)仍低于放射治疗(10.32美元/天)。研究局限性包括数据来源于单一医疗系统,成本基于医疗保险基准估计而非实际支付情况。
对于低风险疾病,2年时主动监测比手术(降低47.6%)和放射治疗(降低68.2%)成本更低,到5年时降低幅度分别为5.6%和37.8%。对于高风险疾病,两个时间段内手术成本均低于放射治疗(分别降低56.1%和59.8%)。