Brain and Vestibular Group, Neuro-Otology Unit, Department of Brain Sciences, Charing Cross Hospital, Imperial College London, London, W6 8RF, UK.
Centre for Neuroimaging Sciences, King's College London, London WC2R 2LS, UK.
Brain. 2021 Feb 12;144(1):128-143. doi: 10.1093/brain/awaa386.
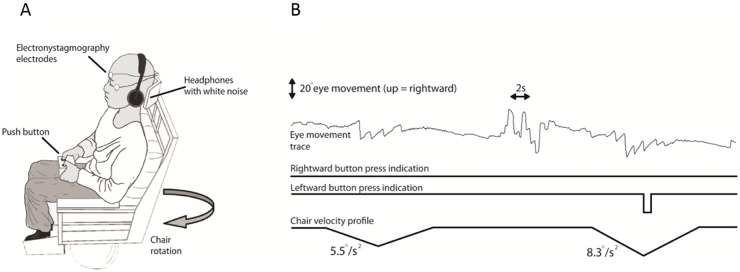
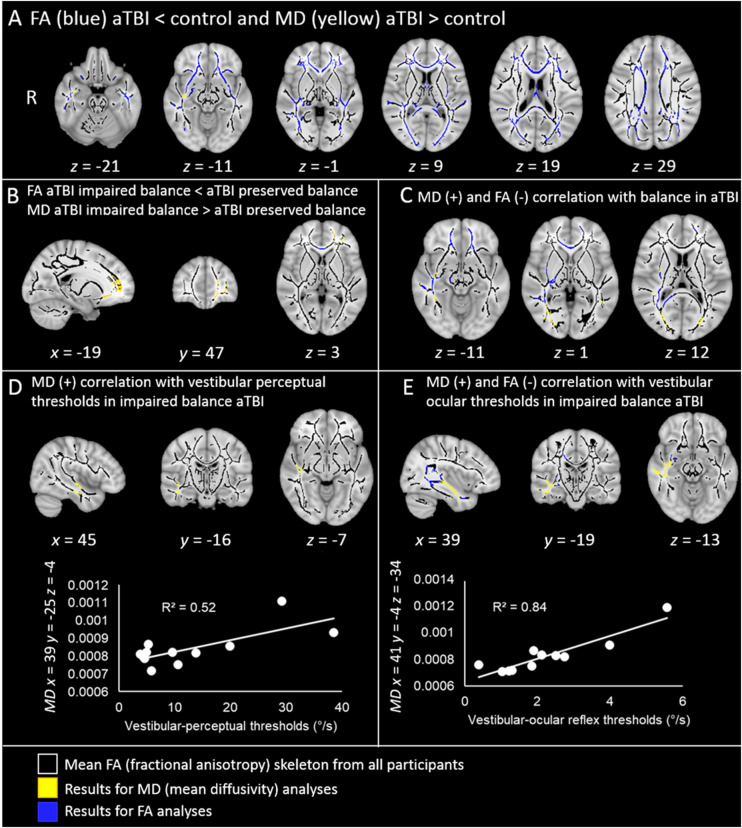
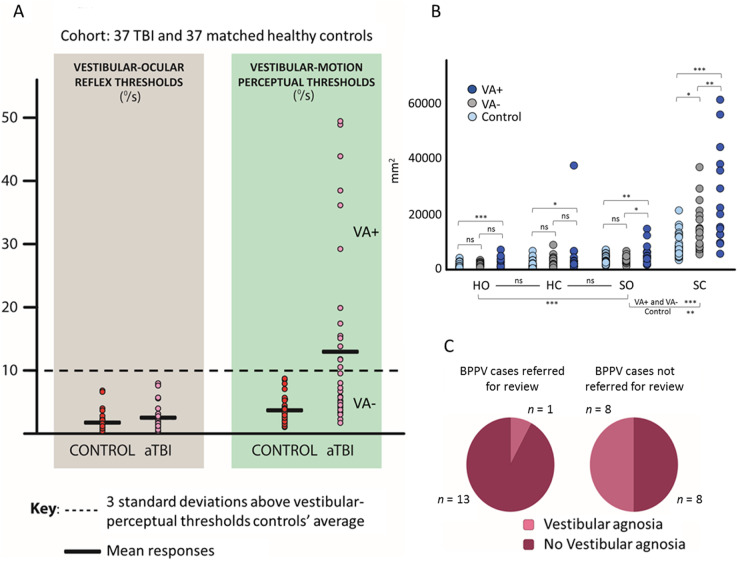
Vestibular dysfunction, causing dizziness and imbalance, is a common yet poorly understood feature in patients with TBI. Damage to the inner ear, nerve, brainstem, cerebellum and cerebral hemispheres may all affect vestibular functioning, hence, a multi-level assessment-from reflex to perception-is required. In a previous report, postural instability was the commonest neurological feature in ambulating acute patients with TBI. During ward assessment, we also frequently observe a loss of vertigo sensation in patients with acute TBI, common inner ear conditions and a related vigorous vestibular-ocular reflex nystagmus, suggesting a 'vestibular agnosia'. Patients with vestibular agnosia were also more unbalanced; however, the link between vestibular agnosia and imbalance was confounded by the presence of inner ear conditions. We investigated the brain mechanisms of imbalance in acute TBI, its link with vestibular agnosia, and potential clinical impact, by prospective laboratory assessment of vestibular function, from reflex to perception, in patients with preserved peripheral vestibular function. Assessment included: vestibular reflex function, vestibular perception by participants' report of their passive yaw rotations in the dark, objective balance via posturography, subjective symptoms via questionnaires, and structural neuroimaging. We prospectively screened 918 acute admissions, assessed 146 and recruited 37. Compared to 37 matched controls, patients showed elevated vestibular-perceptual thresholds (patients 12.92°/s versus 3.87°/s) but normal vestibular-ocular reflex thresholds (patients 2.52°/s versus 1.78°/s). Patients with elevated vestibular-perceptual thresholds [3 standard deviations (SD) above controls' average], were designated as having vestibular agnosia, and displayed worse posturography than non-vestibular-agnosia patients, despite no difference in vestibular symptom scores. Only in patients with impaired postural control (3 SD above controls' mean), whole brain diffusion tensor voxel-wise analysis showed elevated mean diffusivity (and trend lower fractional anisotropy) in the inferior longitudinal fasciculus in the right temporal lobe that correlated with vestibular agnosia severity. Thus, impaired balance and vestibular agnosia are co-localized to the inferior longitudinal fasciculus in the right temporal lobe. Finally, a clinical audit showed a sevenfold reduction in clinician recognition of a common peripheral vestibular condition (benign paroxysmal positional vertigo) in acute patients with clinically apparent vestibular agnosia. That vestibular agnosia patients show worse balance, but without increased dizziness symptoms, explains why clinicians may miss treatable vestibular diagnoses in these patients. In conclusion, vestibular agnosia mediates imbalance in traumatic brain injury both directly via white matter tract damage in the right temporal lobe, and indirectly via reduced clinical recognition of common, treatable vestibular diagnoses.
前庭功能障碍导致头晕和平衡失调,是颅脑损伤患者常见但尚未被充分认识的特征。内耳、神经、脑干、小脑和大脑半球的损伤都可能影响前庭功能,因此需要进行多层面评估,包括从反射到感知。在前一份报告中,姿势不稳是颅脑损伤急性患者最常见的神经学特征。在病房评估中,我们还经常观察到急性颅脑损伤患者失去眩晕感,常见的内耳疾病和相关的剧烈前庭眼反射性眼球震颤,提示存在“前庭认知障碍”。有前庭认知障碍的患者也更不稳定;然而,前庭认知障碍与不平衡之间的联系因内耳疾病的存在而变得复杂。我们通过对保留外周前庭功能的患者进行前瞻性实验室前庭功能评估,从反射到感知,研究急性颅脑损伤患者平衡障碍的大脑机制,及其与前庭认知障碍的关系,以及潜在的临床影响。评估包括:前庭反射功能、参与者在黑暗中被动转头时报告的前庭感知、姿势描记术的客观平衡、问卷调查的主观症状以及结构神经影像学。我们前瞻性地筛选了 918 例急性入院患者,评估了 146 例,并招募了 37 例。与 37 名匹配的对照组相比,患者的前庭感知阈值升高(患者为 12.92°/s,而对照组为 3.87°/s),但前庭眼反射阈值正常(患者为 2.52°/s,而对照组为 1.78°/s)。前庭感知阈值升高[高于对照组平均水平 3 个标准差]的患者被指定为有前庭认知障碍,并且与非前庭认知障碍患者相比,他们的姿势描记术更差,尽管前庭症状评分没有差异。只有在姿势控制受损的患者中(高于对照组平均水平 3 个标准差),整个大脑弥散张量体素分析显示右侧颞叶下纵束的平均弥散度升高(和趋势下的分数各向异性降低),与前庭认知障碍的严重程度相关。因此,受损的平衡和前庭认知障碍都定位于右侧颞叶的下纵束。最后,临床审计显示,在有明显临床前庭认知障碍的急性患者中,临床医生对常见外周前庭疾病(良性阵发性位置性眩晕)的识别减少了七倍。前庭认知障碍患者的平衡更差,但头晕症状没有增加,这解释了为什么临床医生可能会错过这些患者可治疗的前庭诊断。总之,前庭认知障碍通过右侧颞叶白质束损伤直接介导颅脑损伤中的平衡障碍,通过减少对常见可治疗性前庭诊断的临床识别间接介导。