Department of Gastroenterolgy, Oslo University Hospital, Ulleval, Norway.
Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
J Crohns Colitis. 2021 Jun 22;15(6):969-979. doi: 10.1093/ecco-jcc/jjaa232.
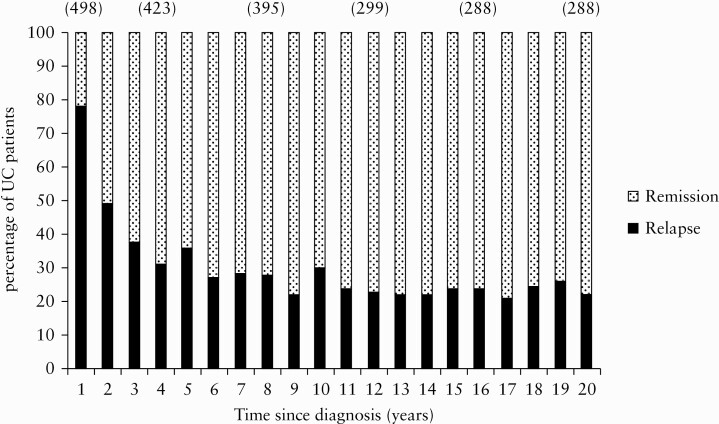
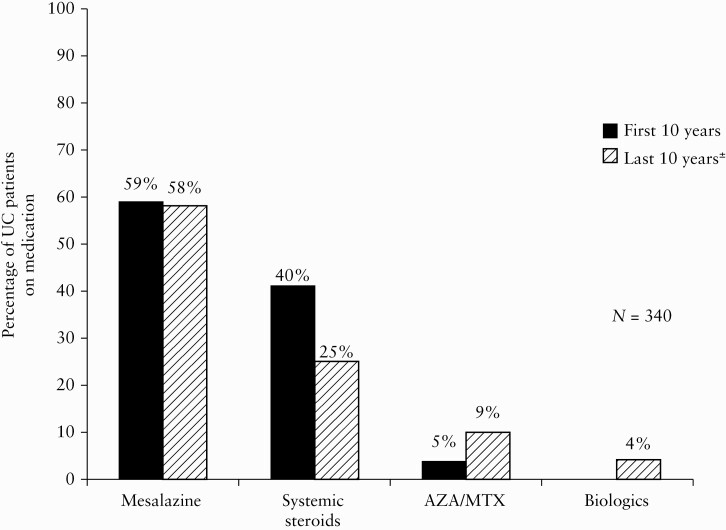
The long-term course of ulcerative colitis [UC] is difficult to predict. Mortality, colectomy, cancer, and hospitalisation represent hard outcomes of disease. Moreover, knowledge on the risk of relapses and need for potent medication add important information about living with UC. We aimed to evaluate the course and prognosis of UC during the first 20 years after diagnosis, and to identify early prognostic risk factors.
From 1990 to 1994, a population-based inception cohort of patients with inflammatory bowel disease was enrolled in South-Eastern Norway. A systematic follow-up [FU] was conducted at 1,5, 10, and 20 years after diagnosis. Clinical outcomes were recorded continuously, and possible relationships between early disease characteristics and outcomes were analysed using multiple regression analysis.
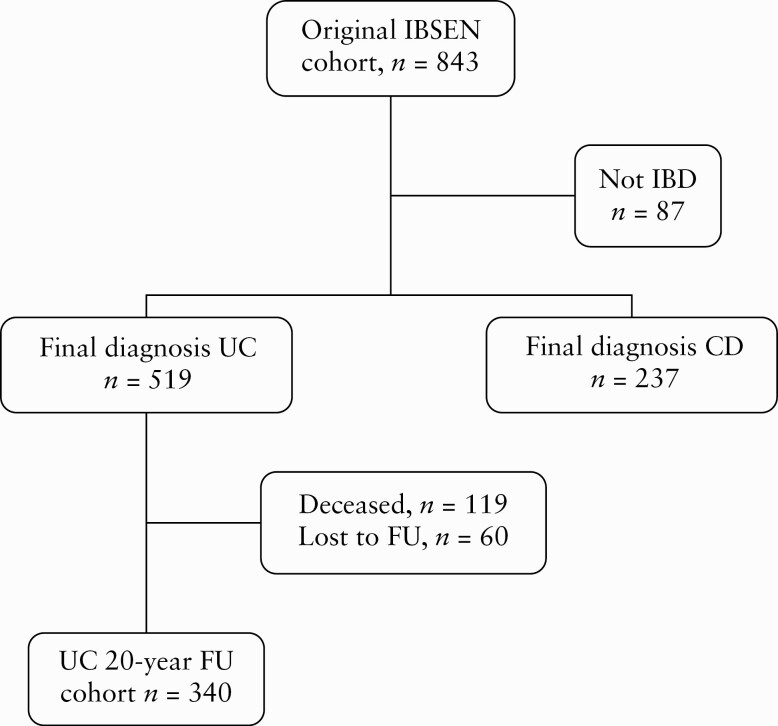
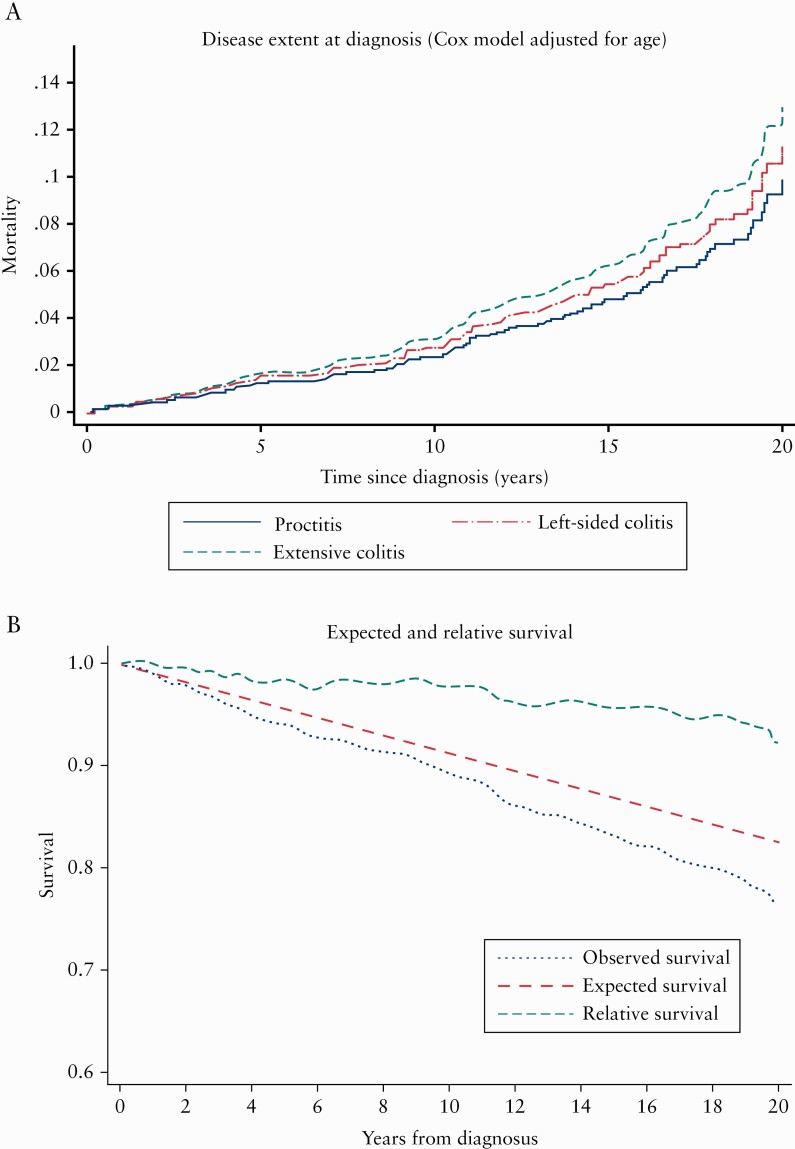
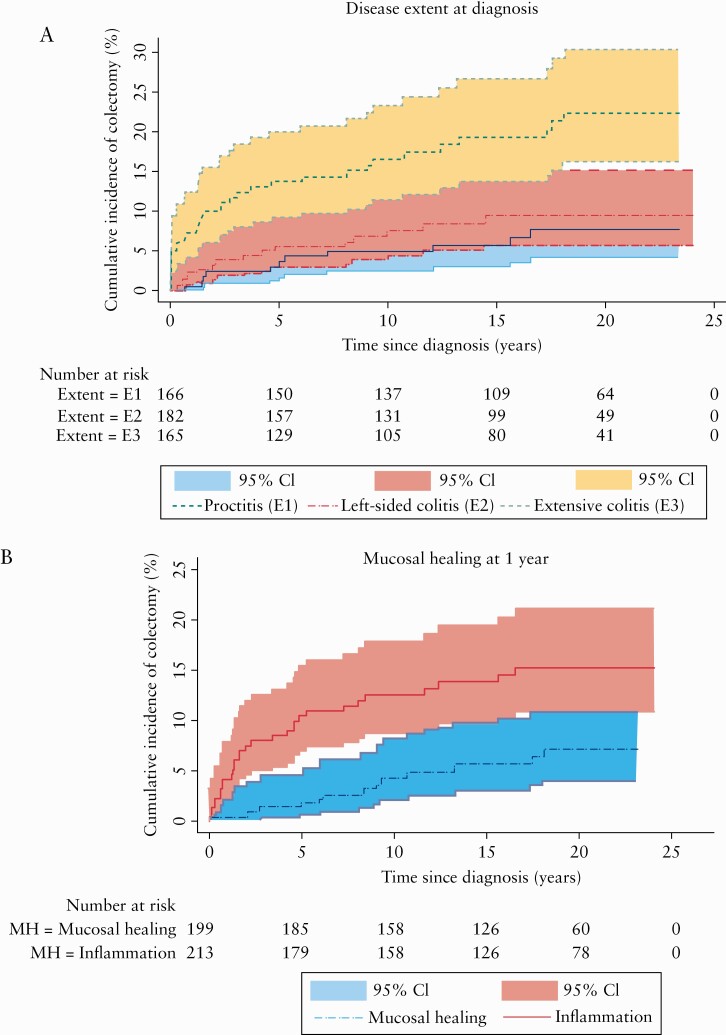
Among 519 UC patients, 119 died, 60 were lost to FU, and 340 were included in the FU cohort. The 20-year cumulative risk of colectomy was 13.0% (95% confidence interval [CI] [11.4-14.6]). Extensive colitis at diagnosis was independently associated with an increased risk of colectomy compared with proctitis (hazard ratio [HR] = 2].8, 95% CI [1.3-6.1]). In contrast, mucosal healing at 1-year FU was independently associated with reduced risk of colectomy [HR = 0.4, 95% CI [0.2-0.8]), and inversely associated with subsequent risk of relapse [adjusted HR = 0.5, 95% CI [0.3-0.7]).
The overall risk of colectomy in our cohort was lower than expected from previous studies, although considerable for patients with extensive colitis at diagnosis. Early mucosal healing was associated with better disease outcomes 20 years after diagnosis.
溃疡性结肠炎(UC)的长期病程难以预测。死亡率、结肠切除术、癌症和住院治疗是疾病的严重后果。此外,了解复发风险和需要强效药物的情况,对于了解 UC 的患者生活状况具有重要意义。本研究旨在评估诊断后 20 年内 UC 的病程和预后,并确定早期预后危险因素。
1990 年至 1994 年,在挪威东南部进行了一项基于人群的炎症性肠病发病队列研究。在诊断后 1、5、10 和 20 年进行系统随访。连续记录临床结局,并使用多元回归分析分析早期疾病特征与结局之间的可能关系。
在 519 例 UC 患者中,119 例死亡,60 例失访,340 例纳入随访队列。20 年累积结肠切除术风险为 13.0%(95%置信区间 [CI] [11.4-14.6])。诊断时为广泛性结肠炎与诊断时为直肠炎相比,结肠切除术风险增加(风险比 [HR] 2.8,95%CI [1.3-6.1])。相反,1 年 FU 时黏膜愈合与结肠切除术风险降低独立相关(HR 0.4,95%CI [0.2-0.8]),与随后的复发风险降低相关(调整 HR 0.5,95%CI [0.3-0.7])。
本队列的总体结肠切除术风险低于以往研究,但对于诊断时为广泛性结肠炎的患者仍然较高。早期黏膜愈合与诊断后 20 年的疾病结局更好相关。