Divisions of Neurocritical Care and Stroke and Cerebrovascular Diseases, Department of Neurology, Brigham and Women's Hospital, Boston, MA, United States.
Center for Neurotechnology and Neurorecovery, Department of Neurology, Massachusetts General Hospital, Boston, MA, United States; Department of Physical Medicine and Rehabilitation, Spaulding Rehabilitation Hospital, Charlestown, MA, United States.
Neuroimage Clin. 2020;28:102503. doi: 10.1016/j.nicl.2020.102503. Epub 2020 Nov 19.
It is not currently possible to predict which patients will develop chronic disorders of consciousness (DoC) after severe traumatic brain injury (TBI). Although the ascending arousal network (AAN) supports human consciousness, it is unknown which AAN pathways must be preserved for patients to recover consciousness.
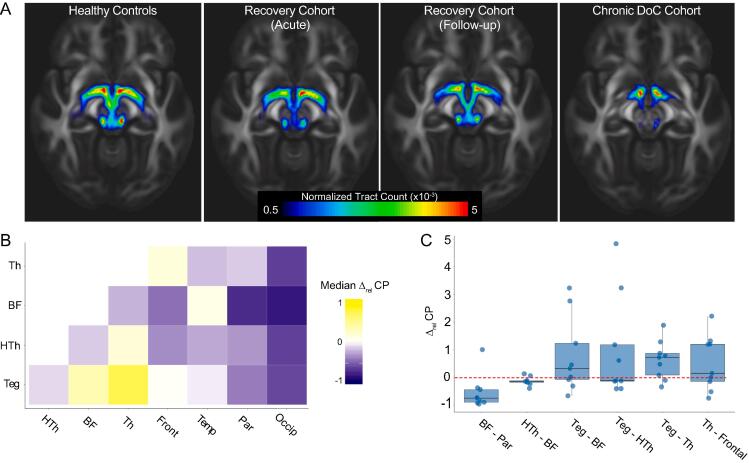
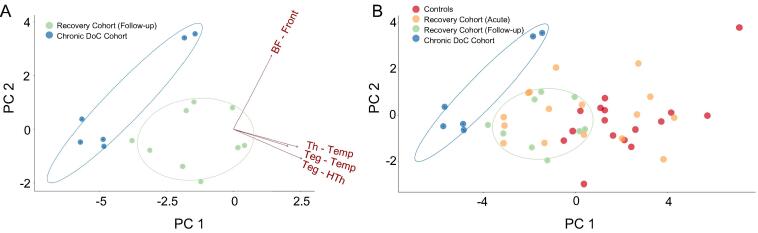
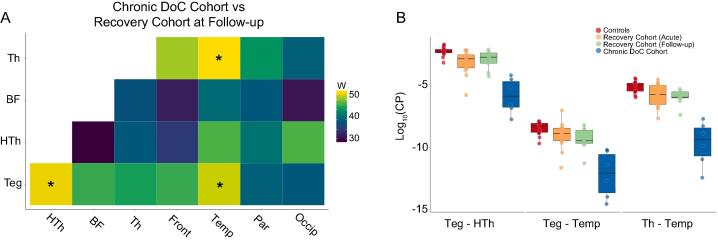
Sixteen patients with acute traumatic coma and 16 matched healthy controls were scanned with high angular resolution diffusion imaging (HARDI). All patients recovered consciousness (Recovery Cohort). Nine were scanned longitudinally: first in the ICU (Acute), then at ≥5 months post-injury (Follow-up). Six separate patients with post-traumatic DoC were scanned ≥5 months post-injury (Chronic DoC Cohort). For each AAN pathway, we computed the median relative change in Acute-to-Follow-up Connectivity Probability (CP) in the Recovery Cohort. We then used Wilcoxon tests with Bonferroni correction to compare CP in each AAN pathway in the Recovery Cohort at Follow-up versus the Chronic DoC Cohort. In an exploratory analysis, we used principal component analysis (PCA) to determine whether linear combinations of AAN CP values could separate the Chronic DoC Cohort from the Recovery Cohort and the healthy controls.
In the Recovery Cohort, the largest relative AAN CP changes were in the brainstem-to-thalamus (median [IQR] = 0.7 [0.09, 0.9]) and forebrain-to-occipital lobe (-0.8 [-0.9, -0.8]) pathways. The AAN connections that differed in the cross-sectional analysis between the Recovery Cohort at Follow-up and the Chronic DoC Cohort included brainstem-to-hypothalamus (W = 53, P = 0.02), brainstem-to-temporal lobe (W = 52, P = 0.04), and thalamus-to-temporal lobe (W = 54, P = 0.009). Plotting the first two principal components of AAN connectivity resulted in a linear separation of Chronic DoC patients from other study groups.
We provide evidence for a longitudinal increase in brainstem-thalamic connectivity during recovery of consciousness after traumatic coma. Cross-sectional analyses revealed that brainstem-hypothalamus, brainstem-temporal lobe, and thalamus-temporal lobe connectivity differed between patients who recovered consciousness and those with a chronic DoC. These observations provide the basis for further investigation into AAN connectivity as a biomarker for recovery of consciousness after traumatic coma.
目前无法预测哪些严重创伤性脑损伤(TBI)患者会出现慢性意识障碍(DoC)。尽管上行觉醒网络(AAN)支持人类意识,但尚不清楚哪些 AAN 通路必须保留,患者才能恢复意识。
对 16 名患有急性创伤性昏迷的患者和 16 名匹配的健康对照组进行高角分辨率弥散成像(HARDI)扫描。所有患者均恢复意识(恢复队列)。9 名患者进行了纵向扫描:首先在 ICU 中(急性期),然后在损伤后≥5 个月(随访期)。另外 6 名患有创伤后慢性 DoC 的患者在损伤后≥5 个月进行了扫描(慢性 DoC 队列)。对于每个 AAN 通路,我们计算了恢复队列中从急性期到随访期的连通性概率(CP)的中位数相对变化。然后,我们使用 Wilcoxon 检验(Bonferroni 校正)比较了恢复队列中每个 AAN 通路在随访期和慢性 DoC 队列中的 CP。在探索性分析中,我们使用主成分分析(PCA)来确定 AAN CP 值的线性组合是否可以将慢性 DoC 队列与恢复队列和健康对照组区分开来。
在恢复队列中,最大的相对 AAN CP 变化发生在脑干-丘脑(中位数[IQR] = 0.7 [0.09, 0.9])和前脑-枕叶(-0.8 [-0.9, -0.8])通路。在横断面分析中,恢复队列随访期与慢性 DoC 队列之间存在差异的 AAN 连接包括脑干-下丘脑(W = 53,P = 0.02)、脑干-颞叶(W = 52,P = 0.04)和丘脑-颞叶(W = 54,P = 0.009)。绘制 AAN 连通性的前两个主成分的图导致慢性 DoC 患者与其他研究组之间的线性分离。
我们提供了在创伤性昏迷后意识恢复过程中脑干-丘脑连通性增加的纵向证据。横断面分析显示,在恢复意识的患者和慢性 DoC 患者之间,脑干-下丘脑、脑干-颞叶和丘脑-颞叶的连通性存在差异。这些观察结果为进一步研究 AAN 连通性作为创伤性昏迷后意识恢复的生物标志物提供了依据。