Schott A M, Termoz A, Viprey M, Tazarourte K, Vecchia C Della, Bravant E, Perreton N, Nighoghossian N, Cakmak S, Meyran S, Ducreux B, Pidoux C, Bony T, Douplat M, Potinet V, Sigal A, Xue Y, Derex L, Haesebaert J
Université de Lyon, Université Claude Bernard Lyon 1 - HESPER EA 7425, 8 Avenue Rockefeller, 69008, Lyon, France.
Hospices Civils de Lyon, Pôle de Sante Publique, Lyon, France.
BMC Health Serv Res. 2021 Jan 4;21(1):12. doi: 10.1186/s12913-020-05982-0.
Optimizing access to recanalization therapies in acute ischemic stroke patients is crucial. Our aim was to measure the short and long term effectiveness, at the acute phase and 1 year after stroke, of four sets of actions implemented in the Rhône County.
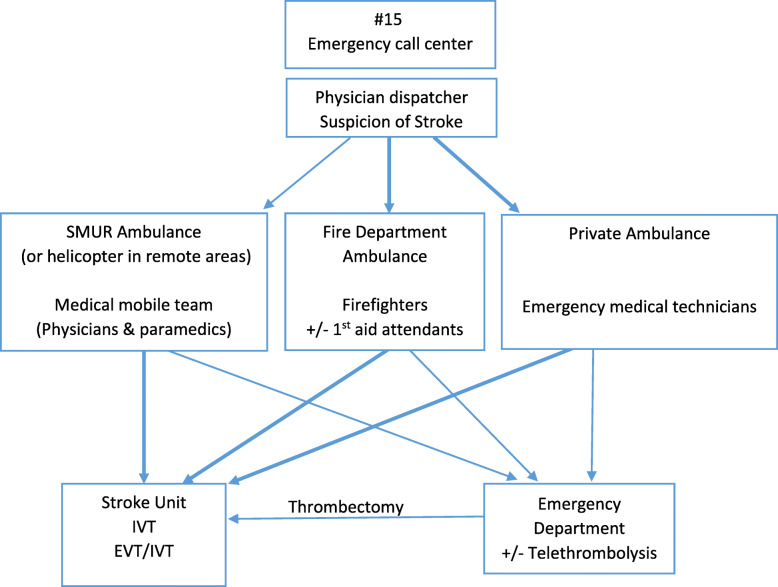
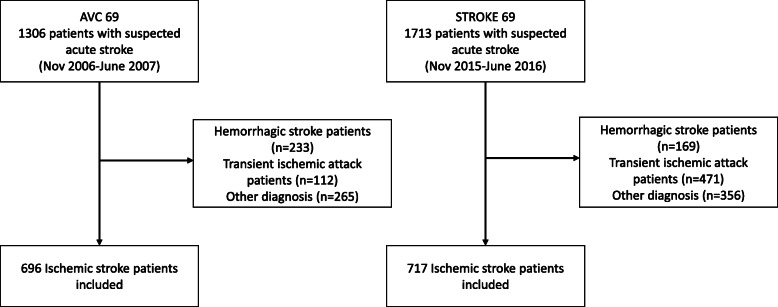
The four multilevel actions were 1) increase in stroke units bed capacity and development of endovascular therapy; 2) improvement in knowledge and skills of healthcare providers involved in acute stroke management using a bottom-up approach; 3) development and implementation of new organizations (transportation routes, pre-notification, coordination by the emergency call center physician dispatcher); and 4) launch of regional public awareness campaigns in addition to national campaigns. A before-and-after study was conducted with two identical population-based cohort studies in 2006-7 and 2015-16 in all adult ischemic stroke patients admitted to any emergency department or stroke unit of the Rhône County. The primary outcome criterion was in-hospital management times, and the main secondary outcome criteria were access to reperfusion therapy (either intravenous thrombolysis or endovascular treatment) and pre-hospital management times in the short term, and 12-month prognosis measured by the modified Rankin Scale (mRS) in the long term.
Between 2015-16 and 2006-7 periods ischemic stroke patients increased from 696 to 717, access to reperfusion therapy increased from 9 to 23% (p < 0.0001), calls to emergency call-center from 40 to 68% (p < 0.0001), first admission in stroke unit from 8 to 30% (p < 0.0001), and MRI within 24 h from 18 to 42% (p < 0.0001). Onset-to-reperfusion time significantly decreased from 3h16mn [2 h54-4 h05] to 2h35mn [2 h05-3 h19] (p < 0.0001), mainly related to a decrease in delay from admission to imaging. A significant decrease of disability was observed, as patients with mild disability (mRS [0-2]) at 12 months increased from 48 to 61% (p < 0.0001). Pre-hospital times, however, did not change significantly.
We observed significant improvement in access to reperfusion therapy, mainly through a strong decrease of in-hospital management times, and in 12-month disability after the implementation of four sets of actions between 2006 and 2016 in the Rhône County. Reducing pre-hospital times remains a challenge.
优化急性缺血性中风患者的再灌注治疗途径至关重要。我们的目的是评估在罗讷省实施的四组行动在中风急性期及中风后1年的短期和长期效果。
这四项多层次行动分别为:1)增加中风单元床位并发展血管内治疗;2)采用自下而上的方法提高参与急性中风管理的医护人员的知识和技能;3)开发并实施新的组织形式(运输路线、预先通知、急救中心医生调度员协调);4)除全国性宣传活动外,开展地区性公众宣传活动。在2006 - 2007年和2015 - 2016年,对所有入住罗讷省任何急诊科或中风单元的成年缺血性中风患者进行了两项相同的基于人群的队列研究,开展了一项前后对照研究。主要结局标准是住院管理时间,主要次要结局标准是短期获得再灌注治疗(静脉溶栓或血管内治疗)的情况和院前管理时间,以及长期采用改良Rankin量表(mRS)测量的12个月预后。
在2015 - 2016年和2006 - 2007年期间,缺血性中风患者从696例增加到717例,获得再灌注治疗的比例从9%增至23%(p < 0.0001),拨打急救中心电话的比例从40%增至68%(p < 0.0001),首次入住中风单元的比例从8%增至30%(p < 0.0001),24小时内进行MRI检查的比例从18%增至42%(p < 0.0001)。从发病到再灌注的时间从3小时16分钟[2小时54 - 4小时05]显著降至2小时35分钟[2小时05 - 3小时19](p < 0.0001),主要是由于从入院到成像的延迟减少。观察到残疾情况显著减少,12个月时轻度残疾(mRS[0 - 2])的患者从48%增至61%(p < 0.0001)。然而,院前时间没有显著变化。
我们观察到,在2006年至2016年罗讷省实施四组行动后,再灌注治疗的可及性有显著改善,主要是通过大幅缩短住院管理时间以及12个月时的残疾情况得到改善。缩短院前时间仍然是一项挑战。