Ocular Oncology Service, Moorfields Eye Hospital NHS Foundation Trust, London, UK
Medical Retina Service, Moorfields Eye Hospital NHS Foundation Trust, London, UK.
Br J Ophthalmol. 2022 Apr;106(4):568-575. doi: 10.1136/bjophthalmol-2020-318095. Epub 2021 Jan 4.
BACKGROUND/AIMS: To describe clinical and multimodal imaging features in a cohort of choroidal macrovessels.
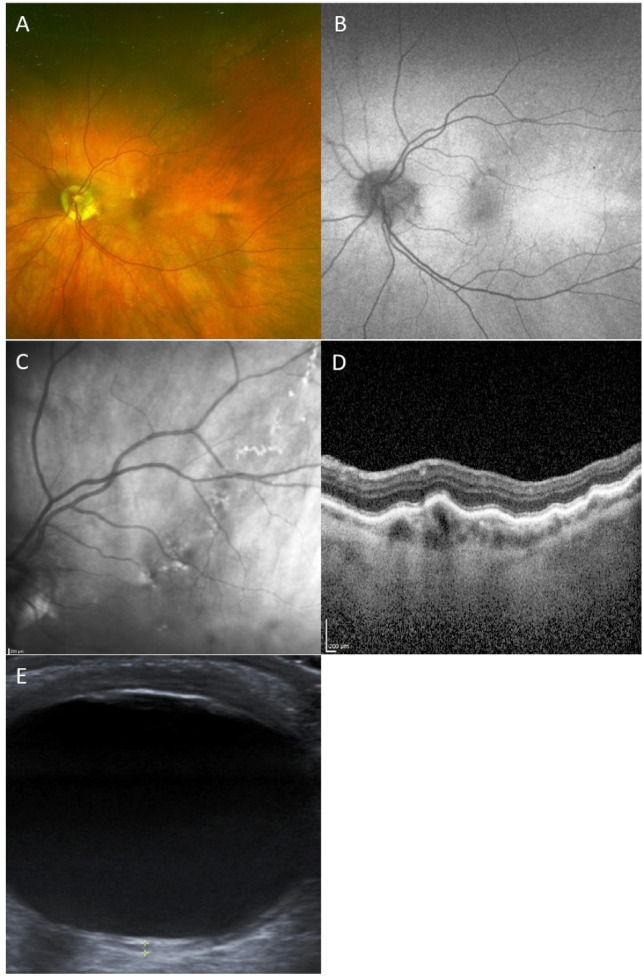
Demographics and multimodal imaging features of 16 eyes of 13 patients with choroidal macrovessels were reviewed. The multimodal imaging included colour fundus photography, fundus autofluorescence (FAF), spectral domain enhanced depth imaging optical coherence tomography (OCT), en face OCT, OCT-angiography (OCT-A), B-scan ultrasonography (US), fluorescein angiography (FFA) and indocyanine green angiography (ICGA).
Three patients had bilateral involvement. On colour fundus photography, three patterns were evident (a clearly visible orange-red vessel; a track of pigmentary changes; spots of mild pigmentary changes). Vessel orientation was horizontal (11 eyes), oblique (4 eyes) or vertical (1 eye). In 2 eyes, the vessel was extra-macular. OCT in all cases showed a hyporeflective choroidal area with posterior shadowing and elevation of the overlying retina. Subretinal fluid was present in 4 eyes. FAF (12 eyes) was normal (7 eyes) or showed a hypofluorescent/hyperfluorescent track (4 eyes) or linear hyperautofluorescence (1 eye). En-face OCT (2 eyes) revealed the course of the macrovessel at the level of choroid and choriocapillaris. On OCT-A (2 eyes) the vessel had a reflectivity similar to surrounding vessels but larger diameter. B-scan US (8 eyes) showed a nodular hypoechogenic lesion. FFA (5 eyes) showed early focal hyperfluorescence (4 eyes) not increasing in later phases, or was normal (1 eye). ICGA (6 eyes) showed early hyperfluorescence of the vessel.
Choroidal macrovessels can mimic other entities, leading to underdiagnosis. Appreciating relevant features on different imaging modalities will aid a correct diagnosis.
背景/目的:描述脉络膜大血管患者队列的临床和多模态成像特征。
回顾了 13 名患者 16 只眼的脉络膜大血管的人口统计学和多模态成像特征。多模态成像包括彩色眼底照相、眼底自发荧光(FAF)、谱域增强深度成像光学相干断层扫描(OCT)、面扫 OCT、OCT 血管造影(OCT-A)、B 型超声扫描(US)、荧光素血管造影(FFA)和吲哚青绿血管造影(ICGA)。
3 名患者为双眼受累。彩色眼底照相显示三种明显的表现(一条清晰可见的橙红色血管;一条脉络膜色素改变的轨迹;一些轻度色素改变的斑点)。血管的方向是水平(11 只眼)、倾斜(4 只眼)或垂直(1 只眼)。在 2 只眼中,血管位于黄斑外。所有病例的 OCT 均显示低反射性脉络膜区域,伴有后影和视网膜上方隆起。4 只眼存在视网膜下液。FAF(12 只眼)正常(7 只眼)或显示低荧光/高荧光轨迹(4 只眼)或线性高自发荧光(1 只眼)。面扫 OCT(2 只眼)显示脉络膜和脉络膜毛细血管水平的大血管的走行。OCT-A(2 只眼)显示血管的反射率与周围血管相似,但直径较大。B 型超声扫描(8 只眼)显示结节状低回声病变。FFA(5 只眼)显示早期局灶性高荧光(4 只眼),后期无增强,或正常(1 只眼)。ICGA(6 只眼)显示早期血管高荧光。
脉络膜大血管可能模仿其他实体,导致漏诊。了解不同成像模式的相关特征将有助于正确诊断。