Hajdu Steven D, Kaesmacher Johannes, Michel Patrik, Sirimarco Gaia, Knebel Jean-Francois, Bartolini Bruno, Kurmann Christoph C, Puccinelli Francesco, Mosimann Pascal J, Bonvin Christophe, Arnold Marcel, Niederhäuser Julien, Eskandari Ashraf, Mordasini Pasquale, Gralla Jan, Fischer Urs, Saliou Guillaume
From the Department of Interventional and Diagnostic Radiology (S.D.H., B.B., F.P., G. Saliou), Department of Neurology (P. Michel, G. Sirimarco, A.E.), and Laboratory for Investigative Neurophysiology (The LINE), Department of Radiology, Department of Clinical Neurosciences, EEG Brain Mapping Core, Centre for Biomedical Imaging (CIBM) (J.-F.K.), Lausanne University Hospital, University of Lausanne; University Institute for Diagnostic, Interventional and Pediatric Radiology (J.K., C.C.K., M.A., U.F.), University Institute for Diagnostic and Interventional Neuroradiology (P.J.M., P. Mordasini, J.G.), University Hospital of Bern, University of Bern; Department of Neurology (C.B.), Sion Hospital; and Department of Neurology (J.N.), Nyon Regional Hospital, Switzerland.
Neurology. 2021 Feb 22;96(8):e1124-e1136. doi: 10.1212/WNL.0000000000011449.
To investigate the association between endovascular therapy (EVT) start time in acute ischemic stroke (AIS) and midterm functional outcome.
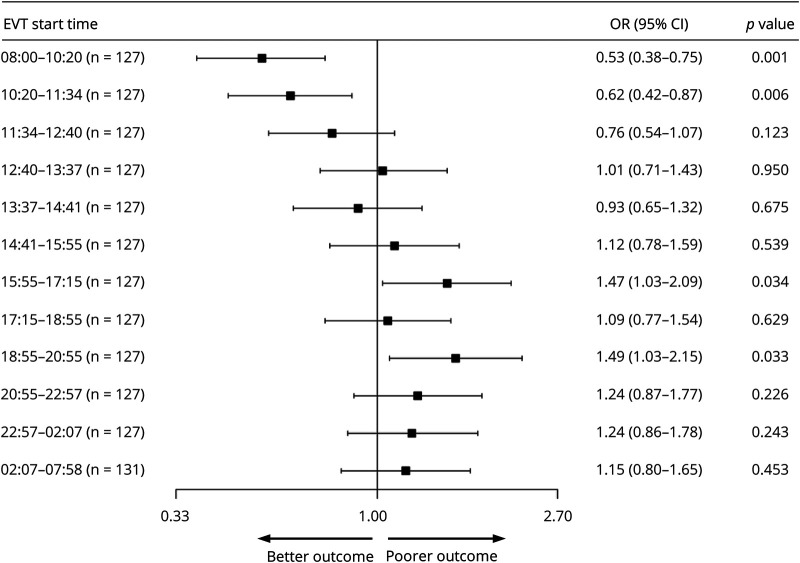
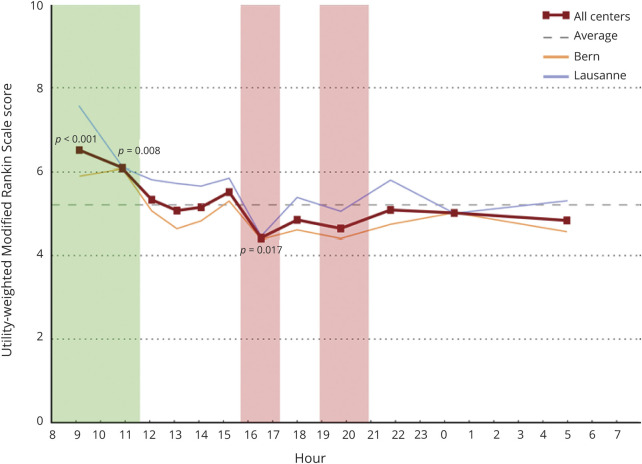
This retrospective cohort study included all patients with AIS treated with EVT from 2 stroke center registries from January 2012 to December 2018. The primary outcome was the score on the modified Rankin Scale (mRS) and the utility-weighted mRS (uw-mRS) at 90 days. A proportional odds model was used to calculate the common odds ratio (OR) as a measure of the likelihood that the intervention at a given EVT start time would lead to lower scores on the mRS (shift analysis).
A total of 1,558 cases were equally allotted into 12 EVT start time periods. The primary outcome favored EVT start times in the morning at 08:00-10:20 and 10:20-11:34 (OR, 0.53; 95% confidence interval [CI], 0.38 to 0.75; < 0.001; OR, 0.62; 95% CI, 0.44 to 0.87; = 0.006, respectively), while it disfavored EVT start times at the end of the working day at 15:55-17:15 and 18:55-20:55 (OR, 1.47; 95% CI, 1.03-2.09; = 0.034; OR, 1.49; 95% CI, 1.03-2.15; = 0.033). Symptom onset to EVT start time was significantly higher and use of IV tissue plasminogen activator significantly lower between 10:20 and 11:34 ( < 0.004 and = 0.012, respectively).
EVT for AIS in the morning leads to better midterm functional outcome, while EVT at the end of the work day leads to poorer midterm functional outcome. Difference in baseline factors, standard workflow, and technical efficacy metrics could not be identified as potential mediators of this effect.
探讨急性缺血性卒中(AIS)血管内治疗(EVT)开始时间与中期功能结局之间的关联。
这项回顾性队列研究纳入了2012年1月至2018年12月期间在2个卒中中心登记处接受EVT治疗的所有AIS患者。主要结局是90天时改良Rankin量表(mRS)评分和效用加权mRS(uw-mRS)评分。采用比例优势模型计算共同优势比(OR),作为在给定EVT开始时间进行干预导致mRS评分降低可能性的一种衡量指标(移位分析)。
总共1558例病例被平均分配到12个EVT开始时间段。主要结局显示,EVT在上午08:00 - 10:20和10:20 - 11:34开始时更具优势(OR分别为0.53;95%置信区间[CI]为0.38至0.75;P < 0.001;OR为0.62;95% CI为0.44至0.87;P = 0.006),而在工作日结束时15:55 - 17:15和18:55 - 20:55进行EVT则不具优势(OR分别为1.47;95% CI为1.03 - 2.09;P = 0.034;OR为1.49;95% CI为1.03 - 2.15;P = 0.033)。在10:20至11:34之间,症状发作至EVT开始时间显著更长,静脉注射组织纤溶酶原激活剂的使用显著更低(分别为P < 0.004和P = 0.012)。
AIS的EVT在上午进行可带来更好的中期功能结局,而在工作日结束时进行EVT则导致较差的中期功能结局。无法确定基线因素、标准工作流程和技术疗效指标的差异是这种效应的潜在介导因素。