State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangdong Key Laboratory of Nasopharyngeal Carcinoma Diagnosis and Therapy, Sun Yat-Sen University Cancer Center, Guangzhou, China; Department of Nasopharyngeal Carcinoma, Sun Yat-Sen University Cancer Center, Guangzhou, China.
State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangdong Key Laboratory of Nasopharyngeal Carcinoma Diagnosis and Therapy, Sun Yat-Sen University Cancer Center, Guangzhou, China; Department of Medical Oncology, Sun Yat-Sen University Cancer Center, Guangzhou, China.
ESMO Open. 2021 Feb;6(1):100004. doi: 10.1016/j.esmoop.2020.100004. Epub 2021 Jan 4.
There is no clinically applicable prognostic model designed for patients with de novo metastatic nasopharyngeal carcinoma (mNPC) treated with chemotherapy followed by locoregional radiotherapy (LRRT). We sought to develop a predictive tool of overall survival for individualized prediction and risk stratification in this heterogeneous patient population.
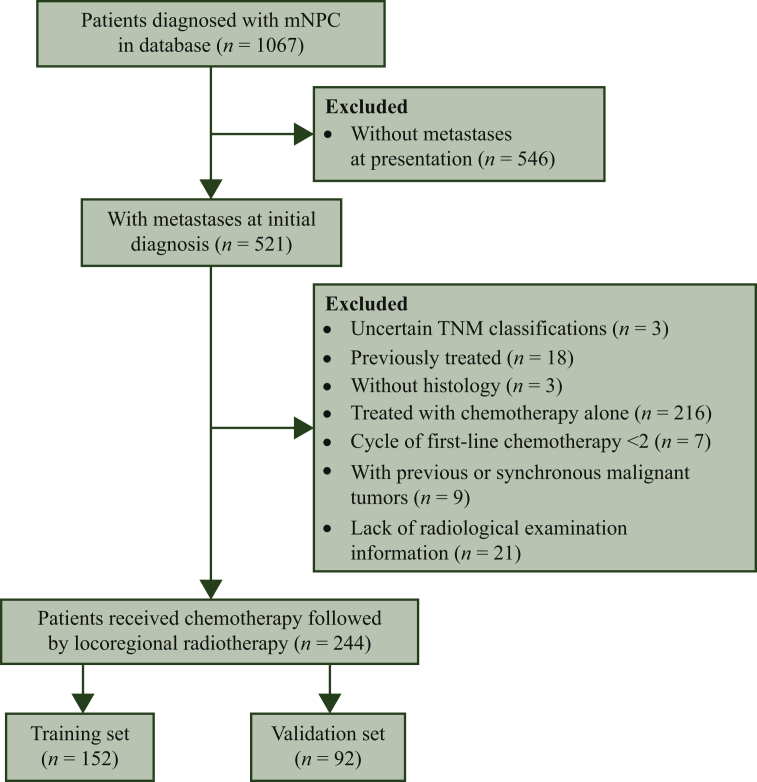
A total of 244 eligible patients with de novo mNPC, who were treated with platinum-based first-line chemotherapy followed by LRRT, were included in this retrospective study. We divided patients into the training and validation sets based on the date of initial treatment, with 152 patients treated between 2008 and 2013 comprising the training set for model development and 92 patients treated at a later time (2014 to 2015) forming the validation set. We applied Cox proportional hazards model to examine factors associated with overall survival (OS). We developed and subsequently validated a prognostic model to predict OS. We assessed the performance of this prognostic model and stratified patients based on prognostic scores obtained from this proposed model.
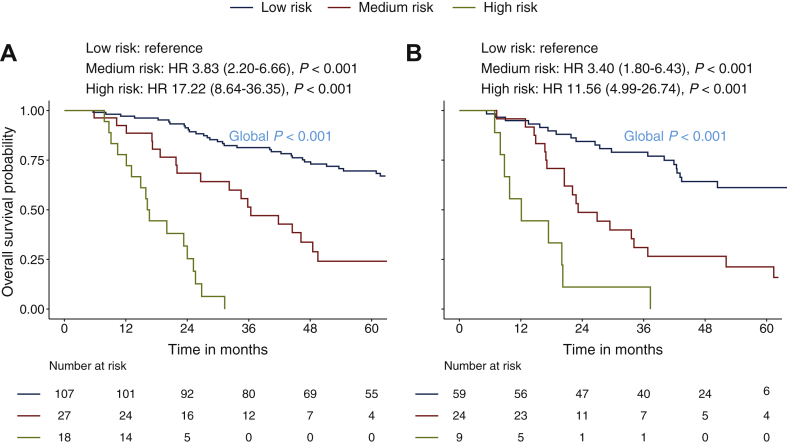
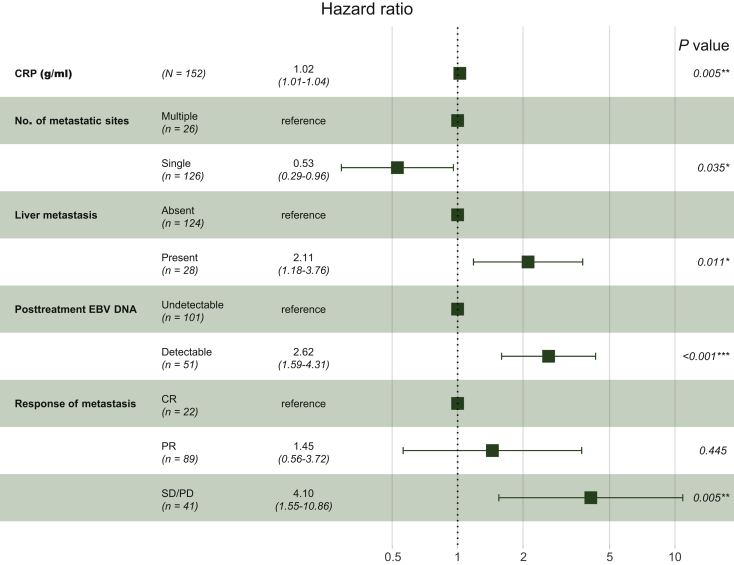
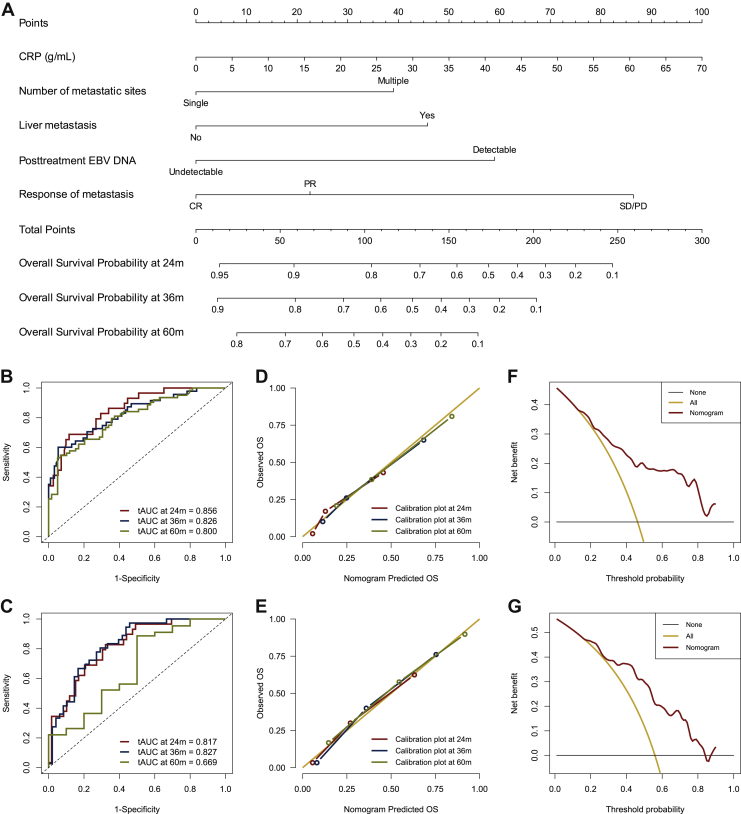
The median OS of the entire cohort was 60.9 months. C-creative protein, number of metastatic sites, liver metastasis, post-treatment Epstein-Barr virus DNA, and response of metastasis were significantly associated with OS. A prognostic model for individual survival prediction was developed and graphically represented as a nomogram. The model showed favorable discrimination (C-index: 0.759), predictive accuracy [time dependent area under the curve (tAUC) at 5 years: 0.800], and calibration, and was further validated in an independent dataset. A risk stratification derived from the model can stratify these patients into three prognostic subgroups with significantly different survival.
We developed and validated a prognostic model that exhibited adequate performance in individualized prediction and risk stratification for patients with de novo mNPC treated with chemotherapy followed by LRRT.
目前尚无针对接受化疗后继以局部区域放疗的初治转移性鼻咽癌(mNPC)患者设计的临床适用的预后模型。我们旨在为这一异质患者群体开发一种总生存的预测工具,以实现个体化预测和风险分层。
这项回顾性研究共纳入 244 例符合条件的初治 mNPC 患者,他们接受铂类为基础的一线化疗后继以局部区域放疗。我们根据初始治疗日期将患者分为训练集和验证集,其中 152 例患者于 2008 年至 2013 年期间接受治疗,构成模型开发的训练集,92 例患者于较晚时间(2014 年至 2015 年)接受治疗,构成验证集。我们应用 Cox 比例风险模型来检验与总生存(OS)相关的因素。我们开发了一个预测模型,并随后对其进行验证,以预测 OS。我们评估了该预后模型的性能,并根据该模型获得的预后评分对患者进行分层。
整个队列的中位 OS 为 60.9 个月。C-反应蛋白、转移部位数量、肝转移、治疗后 EBV-DNA 以及转移灶的反应与 OS 显著相关。我们开发了一个用于个体生存预测的预后模型,并以列线图的形式呈现。该模型显示出良好的区分度(C 指数:0.759)、预测准确性[5 年时间依赖性曲线下面积(tAUC):0.800]和校准能力,并在独立数据集得到了进一步验证。从模型中得出的风险分层可以将这些患者分为具有显著不同生存的三个预后亚组。
我们开发并验证了一个预后模型,该模型在接受化疗后继以局部区域放疗的初治 mNPC 患者的个体化预测和风险分层方面表现出良好的性能。