Harris Andrew B, Zhang Bo, Marrache Majd, Puvanesarajah Varun, Raad Micheal, Hassanzadeh Hamid, Bicket Mark, Jain Amit
Department of Orthopaedic Surgery, The Johns Hopkins University, Baltimore, MD, USA.
Department of Orthopaedic Surgery, University of Virginia, Charlottesville, VA, USA.
Neurospine. 2020 Dec;17(4):879-887. doi: 10.14245/ns.2040122.061. Epub 2020 Dec 31.
Lumbar discectomy is commonly performed for symptomatic lumbar disc herniation. We aimed to examine prescribing patterns and risk factors for chronic opioid use following lumbar discectomy.
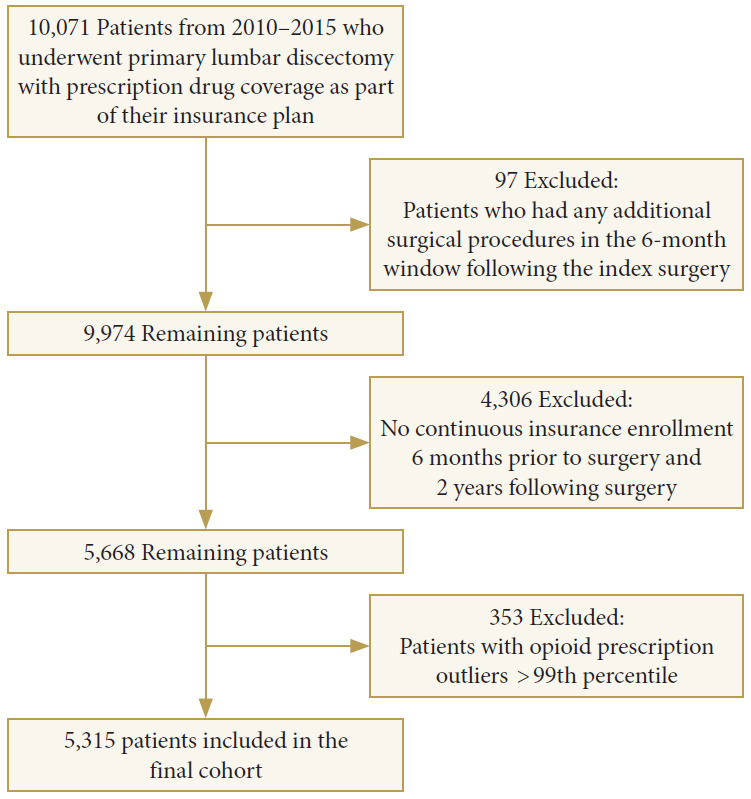
Using a private insurance claims database, patients were identified who underwent primary lumbar discectomy from 2010-2015 and had 1-year of continuous enrollment postoperatively. Patients were excluded with spinal fusion. The strength of opioid prescriptions was quantified using morphine milligram equivalents daily (MMED). Univariate and multivariate logistic regression models were built to examine risk factors associated with chronic postoperative opioid use.
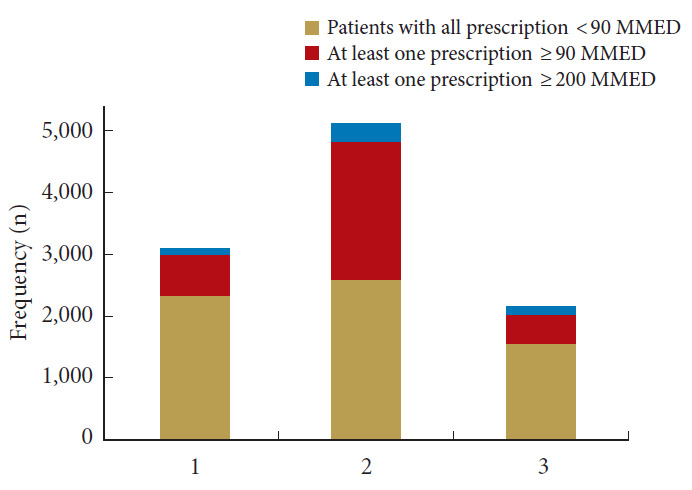
A total of 5,315 patients were included in the study (mean age, 59 years; 50% female). 1,198 of patients (23%) used chronic opioids postoperatively. Chronic opioid use declined significantly from 27% in 2010 to 17% in 2015, p < 0.001. In addition, there were significantly fewer patients receiving high and very high-dose opioid prescriptions from 2010-2015, p < 0.001. The median duration that patients used opioids postoperatively was 211 days in 2010 (interquartile range [IQR], 29-356 days), and decreased significantly to 44 days (IQR, 10-294 days) in 2015. The strongest factors associated with chronic opioid use were preoperative opioid use (odds ratio [OR], 4.0), drug abuse (OR, 2.6), depression (OR, 1.6), surgery in the west (OR, 1.6) or south (OR, 1.6), anxiety (OR, 1.5), or 30-day readmission (OR, 1.4).
Chronic opioid use following primary lumbar discectomy has declined from 2010-2015. A variety of factors are associated with chronic opioid use. Preoperative recognition of some of these risk factors may aid in perioperative management and counseling.
腰椎间盘切除术常用于治疗有症状的腰椎间盘突出症。我们旨在研究腰椎间盘切除术后慢性阿片类药物使用的处方模式和风险因素。
利用一个私人保险理赔数据库,确定了2010年至2015年接受初次腰椎间盘切除术且术后连续参保1年的患者。排除接受脊柱融合术的患者。使用每日吗啡毫克当量(MMED)对阿片类药物处方强度进行量化。构建单因素和多因素逻辑回归模型,以研究与术后慢性阿片类药物使用相关的风险因素。
共有5315例患者纳入研究(平均年龄59岁;50%为女性)。1198例患者(23%)术后使用慢性阿片类药物。慢性阿片类药物的使用从2010年的27%显著下降至2015年的17%,p<0.001。此外,2010年至2015年期间,接受高剂量和非常高剂量阿片类药物处方的患者明显减少,p<0.001。2010年患者术后使用阿片类药物的中位持续时间为211天(四分位间距[IQR],29 - 356天),到2015年显著降至44天(IQR,10 - 294天)。与慢性阿片类药物使用相关的最强因素包括术前阿片类药物使用(比值比[OR],4.0)、药物滥用(OR,2.6)、抑郁症(OR,1.6)、在西部(OR,1.6)或南部(OR,1.6)进行手术、焦虑症(OR,1.5)或30天内再次入院(OR,1.4)。
2010年至2015年期间,初次腰椎间盘切除术后慢性阿片类药物的使用有所下降。多种因素与慢性阿片类药物使用相关。术前识别其中一些风险因素可能有助于围手术期管理和咨询。