Division of Nephrology, Department of Internal Medicine, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan.
Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan.
Crit Care. 2021 Jan 5;25(1):5. doi: 10.1186/s13054-020-03434-z.
Acute kidney injury (AKI) is a common yet possibly fatal complication among critically ill patients in intensive care units (ICU). Although renal replacement therapy (RRT) is an important supportive management for severe AKI patients, the optimal timing of RRT initiation for these patients is still unclear.
In this systematic review, we searched all relevant randomized controlled trials (RCTs) that directly compared accelerated with standard initiation of RRT from PUBMED, MEDLINE, EMBASE, and Cnki.net published prior to July, 20, 2020. We extracted study characteristics and outcomes of being free of dialysis, dialysis dependence and mortality. We rated the certainty of evidence according to Cochrane methods and the GRADE approach.
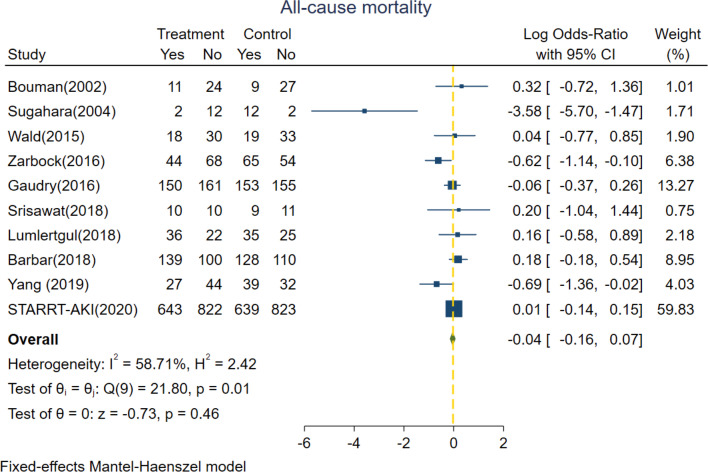
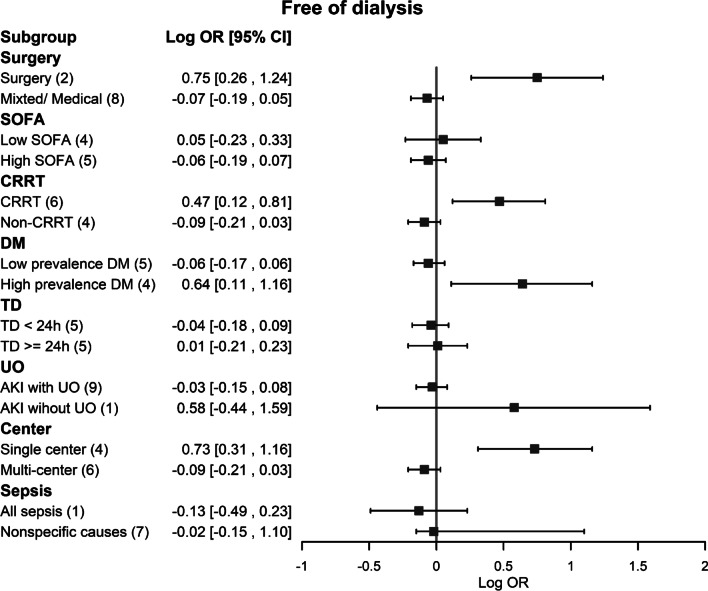
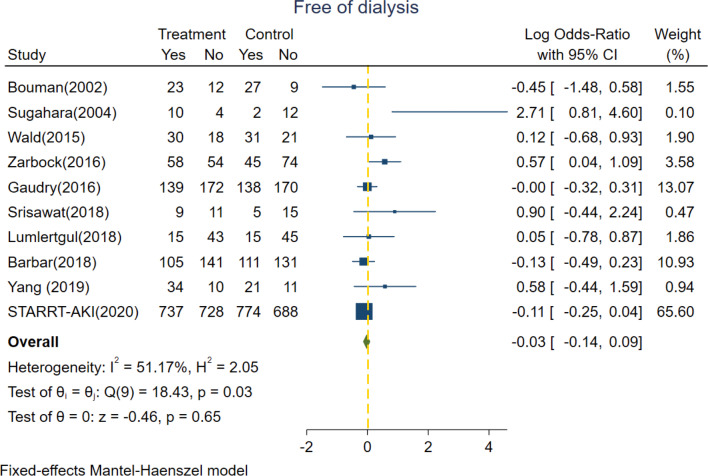
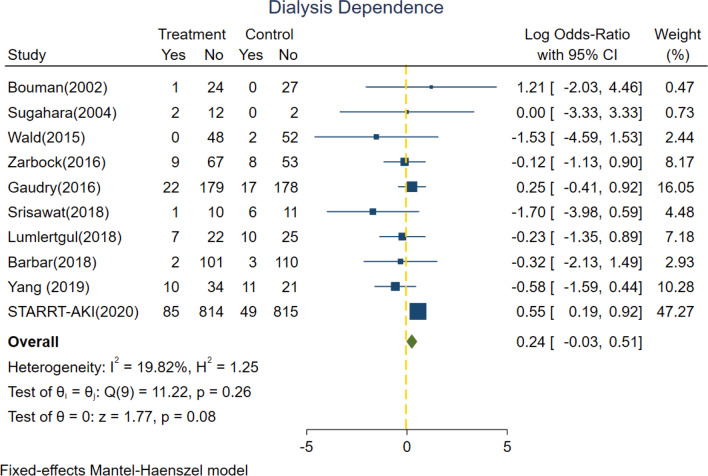
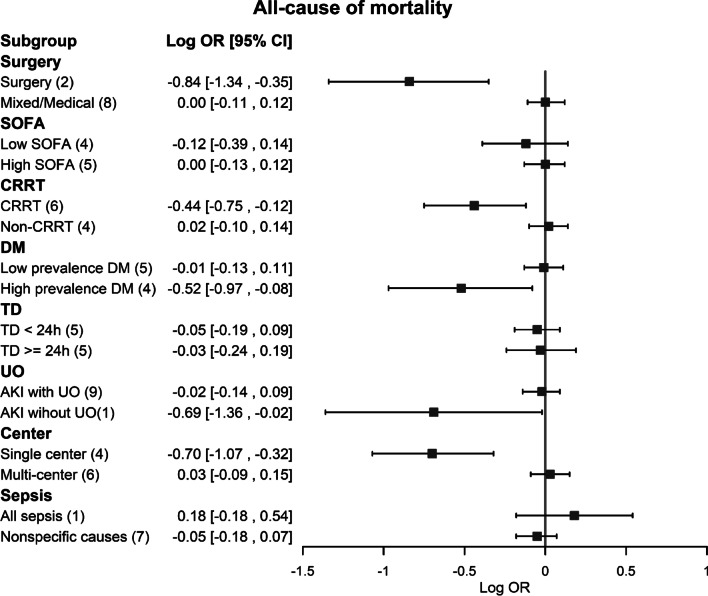
We identified 56 published relevant studies from 1071 screened abstracts. Ten RCTs with 4753 critically ill AKI patients in intensive care unit (ICU) were included in this meta-analysis. In our study, accelerated and standard RRT group were not associated with all-cause mortality (log odds-ratio [OR]: - 0.04, 95% confidence intervals [CI] - 0.16 to 0.07, p = 0.46) and free of dialysis (log OR: - 0.03, 95% CI - 0.14 to 0.09, p = 0.65). In the subgroup analyses, accelerated RRT group was significantly associated with lower risk of all-cause mortality in the surgical ICU and for those who received continuous renal replacement therapy (CRRT). In addition, patients in these two subgroups had higher chances of being eventually dialysis-free. However, accelerated initiation of RRT augmented the risk of dialysis dependence in the subgroups of patients treated with non-CRRT modality and whose Sequential Organ Failure Assessment (SOFA) score were more than 11.
In this meta-analysis, critically ill patients with severe AKI would benefit from accelerated RRT initiation regarding all-cause mortality and being eventually free of dialysis only if they were surgical ICU patients or if they underwent CRRT treatment. However, the risk of dialysis dependence was increased in the accelerated RRT group when those patients used non-CRRT modality or had high SOFA scores. All the literatures reviewed in this study were highly heterogeneous and potentially subject to biases. Trial registration CRD42020201466, Sep 07, 2020. https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=201466 .
急性肾损伤(AKI)是重症监护病房(ICU)中危重病患者常见且可能致命的并发症。虽然肾脏替代治疗(RRT)是严重 AKI 患者的重要支持治疗方法,但这些患者开始 RRT 的最佳时机仍不清楚。
在这项系统评价中,我们从 PUBMED、MEDLINE、EMBASE 和 Cnki.net 搜索了所有直接比较加速与标准开始 RRT 的相关随机对照试验(RCT),这些 RCT 的发表时间均在 2020 年 7 月 20 日之前。我们提取了无透析、依赖透析和死亡率的研究特征和结局。我们根据 Cochrane 方法和 GRADE 方法对证据的确定性进行了评级。
我们从 1071 篇筛选摘要中确定了 56 篇已发表的相关研究。这项荟萃分析纳入了 10 项 RCT,共纳入了 4753 例 ICU 中患有 AKI 的危重病患者。在我们的研究中,加速和标准 RRT 组与全因死亡率(对数优势比 [OR]:-0.04,95%置信区间 [CI]:-0.16 至 0.07,p=0.46)和无透析(对数 OR:-0.03,95%CI:-0.14 至 0.09,p=0.65)无关。在亚组分析中,加速 RRT 组在外科 ICU 和接受连续肾脏替代治疗(CRRT)的患者中,全因死亡率的风险显著降低。此外,这两个亚组的患者最终无透析的可能性更高。然而,在接受非 CRRT 模式治疗和 SOFA 评分大于 11 的患者亚组中,加速开始 RRT 增加了依赖透析的风险。
在这项荟萃分析中,严重 AKI 的危重病患者如果是外科 ICU 患者或接受 CRRT 治疗,则从加速 RRT 开始治疗中获益,可降低全因死亡率和最终无透析的风险。然而,在使用非 CRRT 模式或 SOFA 评分较高的患者中,加速 RRT 组的透析依赖风险增加。本研究综述的所有文献均高度异质,可能存在偏倚。试验注册 CRD42020201466,2020 年 9 月 7 日。https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=201466 。