Korkmaz Ekren Pervin, Öztürk Pelin, Ertugay Serkan, Özdil Ali, Nalbantgil Sanem, Engin Çağatay, Yağdı Tahir, Özbaran Mustafa
Department of Chest Diseases, Ege University Medical Faculty, Izmir, Turkey.
Department of Cardiovascular Surgery, Ege University Medical Faculty, Izmir, Turkey.
Turk Gogus Kalp Damar Cerrahisi Derg. 2020 Oct 21;28(4):576-585. doi: 10.5606/tgkdc.dergisi.2020.19768. eCollection 2020 Oct.
This study aims to investigate the effect of low percentage of forced vital capacity measured in the preoperative period on the 28-day mortality in patients undergoing left ventricular assist device implantation.
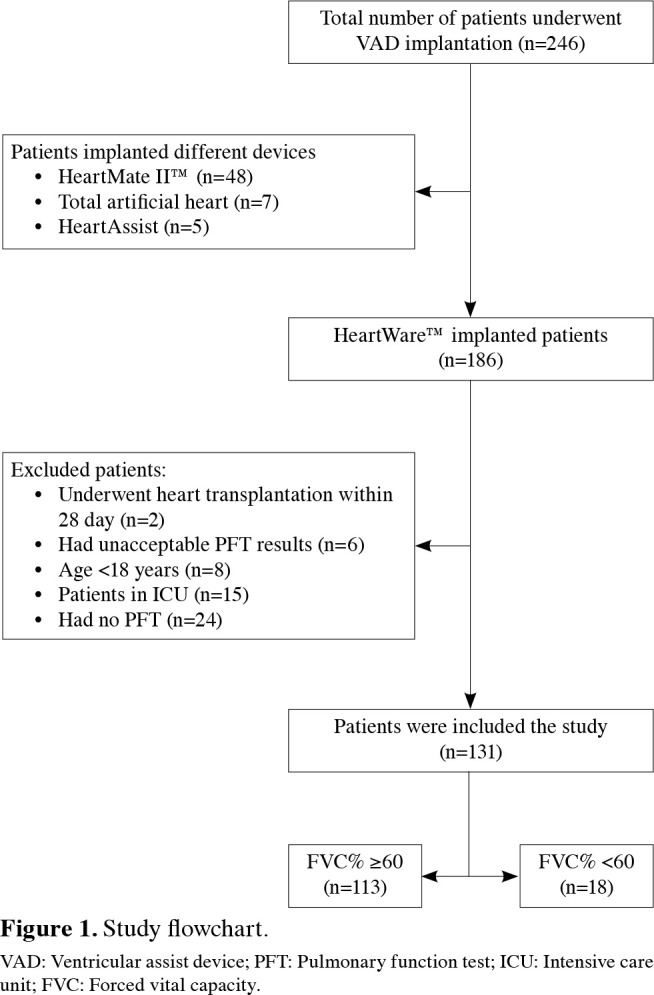
A total of 131 patients (111 males, 20 females; median age 54 years; range, 47 to 59 years) who underwent left ventricular assist device implantation with HeartWare™ between December 2010 and January 2016 were retrospectively analyzed. The patients were divided into two groups according to the results of pulmonary function test as a forced vital capacity percentage of ≥60% (n=113) and <60% (n=18). Both groups were compared in terms of laboratory and clinical characteristics, and postoperative complications. Risk factors for postoperative 28-day mortality were analyzed.
Pre- and intraoperative characteristics were similar in both groups, except for left ventricular end-diastolic diameter. The ventilator-free days up to 28 days was shorter (p=0.046) and the length of intensive care unit stay was longer (p=0.011) in the low percentage of forced vital capacity group. The 28-day mortality rate was also higher (22.2% vs. 9.7%, respectively; p=0.12) in this group. The history of prior cardiac operation (odds ratio: 4.40; 95% confidence interval 1.19-16.20, p=0.026) and tricuspid valve repair at the time of device implantation (odds ratio: 5.30; 95% confidence interval 1.33-21.00, p=0.018) were found to be independent risk factors for mortality. Multivariate analysis showed that a forced vital capacity of <60% was not associated with mortality (odds ratio: 3.96; 95% confidence interval 0.95-16.43, p=0.058).
The length of intensive care unit stay and duration of mechanical ventilation may be longer in patients with a low percentage of forced vital capacity. Although the association between 28-day mortality and low percentage of forced vital capacity is not significant, the risk of 28-day mortality is higher in this group. Therefore, the patients should be assessed carefully before the left ventricular assist device operation.
本研究旨在探讨术前测得的低百分比用力肺活量对接受左心室辅助装置植入患者28天死亡率的影响。
回顾性分析2010年12月至2016年1月期间使用HeartWare™进行左心室辅助装置植入的131例患者(111例男性,20例女性;中位年龄54岁;范围47至59岁)。根据肺功能测试结果将患者分为两组,用力肺活量百分比≥60%(n = 113)和<60%(n = 18)。比较两组的实验室和临床特征以及术后并发症。分析术后28天死亡率的危险因素。
除左心室舒张末期直径外,两组术前和术中特征相似。用力肺活量百分比低的组28天内无呼吸机天数较短(p = 0.046),重症监护病房住院时间较长(p = 0.011)。该组28天死亡率也较高(分别为22.2%和9.7%;p = 0.12)。既往心脏手术史(比值比:4.40;95%置信区间1.19 - 16.20,p = 0.026)和装置植入时三尖瓣修复(比值比:5.30;95%置信区间1.33 - 21.00,p = 0.018)被发现是死亡的独立危险因素。多因素分析显示,用力肺活量<60%与死亡率无关(比值比:3.96;95%置信区间0.95 - 16.43,p = 0.058)。
用力肺活量百分比低的患者重症监护病房住院时间和机械通气时间可能更长。虽然28天死亡率与低百分比用力肺活量之间的关联不显著,但该组28天死亡风险更高。因此,在左心室辅助装置手术前应对患者进行仔细评估。