Ormsby Jennifer, Conrad Paula, Blumenthal Jennifer, Carpenter Jane, Jones Sarah, Sandora Thomas J, Vaughan Ana, Vincuilla Julie, McAdam Alexander J, Fogg Louis F, Flett Kelly, Kelly Daniel P
Boston Children's Hospital, Boston, Mass.
Department of Pediatrics, Boston Children's Hospital and Harvard Medical School, Boston, Mass.
Pediatr Qual Saf. 2020 Dec 28;6(1):e368. doi: 10.1097/pq9.0000000000000368. eCollection 2021 Jan-Feb.
There is no consensus definition for ventilator-associated tracheitis and limited evidence to guide diagnosis and treatment. To improve acute tracheitis evaluation and management, this quality improvement project aimed to (1) improve the appropriateness of tracheal aspirate cultures while decreasing the number of unnecessary cultures by 20% and (2) decrease antibiotic use for acute tracheitis not consistent with local guidelines by 20% over 12 months among pediatric patients requiring mechanical ventilation.
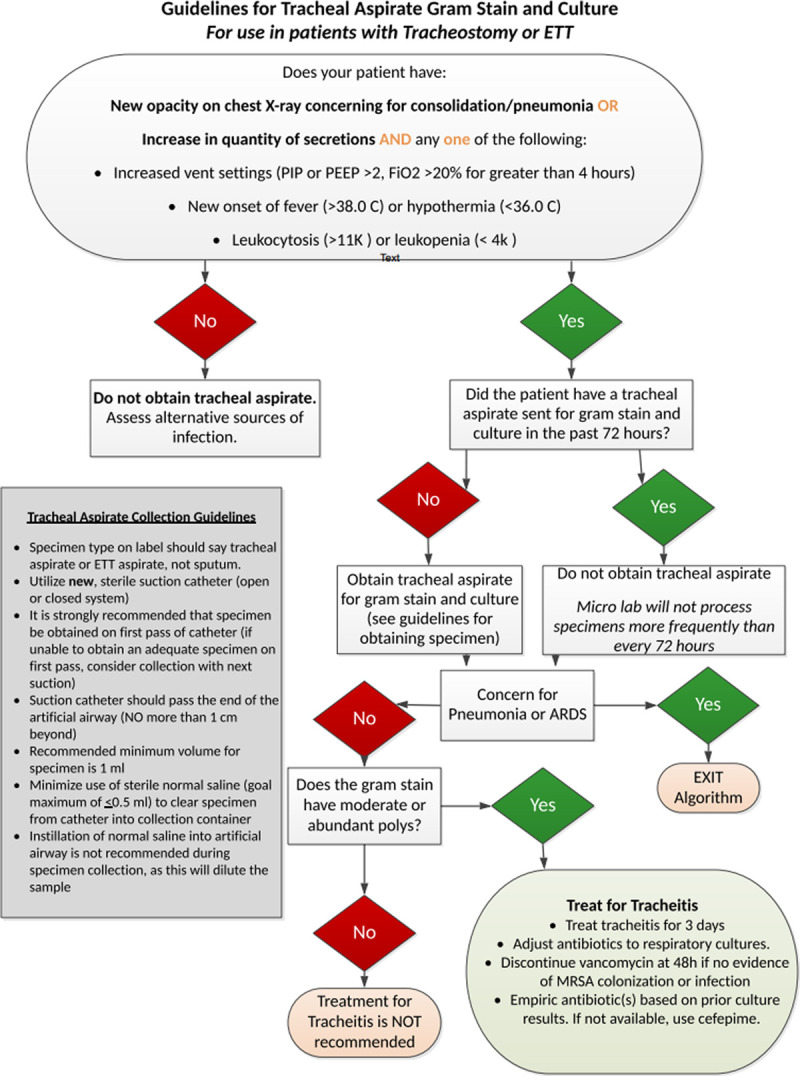
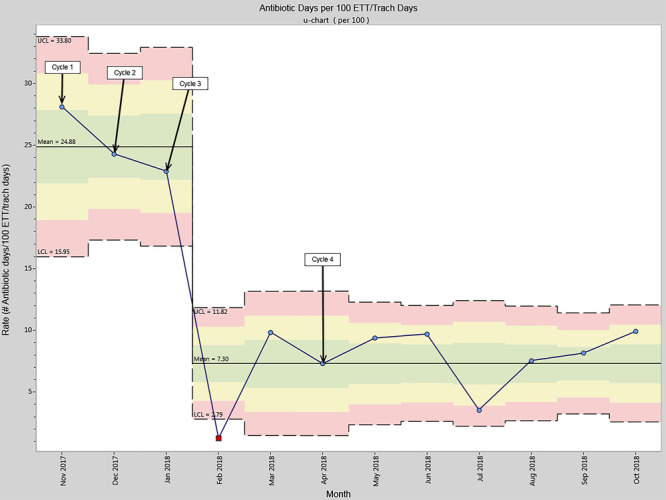
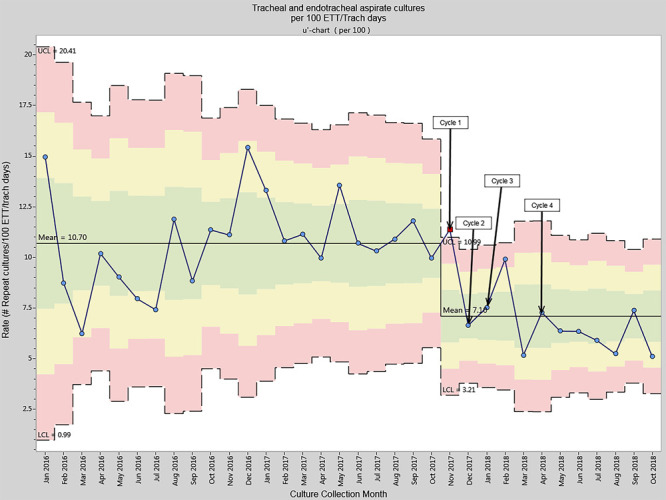
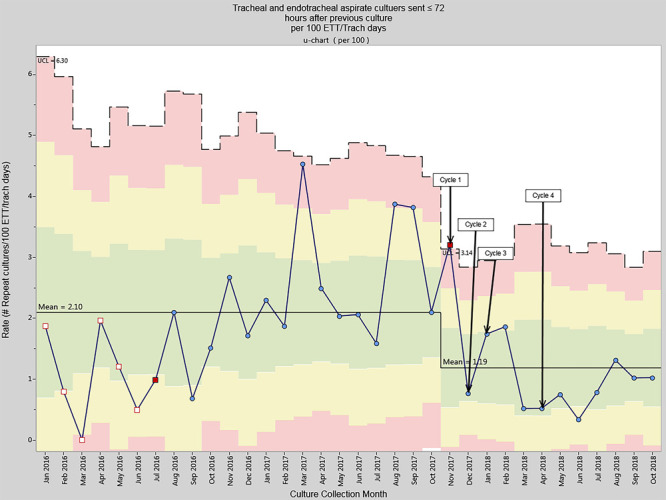
All patients admitted to the Medical Intensive Care Unit requiring mechanical ventilation via an artificial airway were included. Tracheal aspirate sampling criteria, technique, and minimum intervals were standardized. Primary outcome measures were the number of tracheal aspirate cultures obtained per 100 ETT/tracheostomy days and ventilator-associated antibiotic days per 100 ETT/tracheostomy days. Improvement cycles included: Implementation of tracheal aspirate sampling criteria, sampling technique standardization, limiting repeat cultures to >72-hour intervals, and standardizing empiric antibiotic therapy.
Tracheal aspirate culture rate decreased from 10.70 to 7.10 cultures per 100 ETT/tracheostomy days ( < 0.001). Cultures meeting sampling criteria increased from 28% to 80%. Ventilator-associated antibiotic use decreased from 24.88 to 7.30 ventilator-associated antibiotic days per 100 ETT/tracheostomy days. There were no associated increases in ventilator-associated events or days of mechanical ventilation.
Implementation of standardized criteria for tracheal aspirate sampling, improved tracheal aspirate sampling technique, limiting repeat tracheal aspirate cultures, and utilizing standardized antibiotic treatment guidelines safely decreased resource utilization and antibiotic use among critically ill children requiring mechanical ventilation.
对于呼吸机相关性气管炎症,目前尚无共识性定义,且指导诊断和治疗的证据有限。为改善急性气管炎症的评估和管理,本质量改进项目旨在:(1)提高气管吸出物培养的合理性,同时将不必要培养的数量减少20%;(2)在12个月内,使不符合当地指南的急性气管炎症患儿接受机械通气时的抗生素使用量减少20%。
纳入所有入住医学重症监护病房、需通过人工气道进行机械通气的患者。气管吸出物采样标准、技术和最短间隔时间均实现标准化。主要结局指标为每100个气管内插管/气管造口术日获得的气管吸出物培养次数,以及每100个气管内插管/气管造口术日的呼吸机相关性抗生素使用天数。改进周期包括:实施气管吸出物采样标准、采样技术标准化、将重复培养限制在间隔>72小时,以及经验性抗生素治疗标准化。
气管吸出物培养率从每100个气管内插管/气管造口术日10.70次降至7.10次(<0.001)。符合采样标准的培养次数从28%增至80%。每100个气管内插管/气管造口术日的呼吸机相关性抗生素使用天数从24.88天降至7.30天。呼吸机相关性事件或机械通气天数未出现相应增加。
实施标准化的气管吸出物采样标准、改进气管吸出物采样技术、限制重复气管吸出物培养,并采用标准化抗生素治疗指南,可安全降低需要机械通气的危重症患儿的资源利用和抗生素使用。