Princess Máxima Center for Pediatric Oncology, Utrecht, the Netherlands.
Center of Bioinformatics, Biostatistics and Bioimaging, University of Milano-Bicocca, Monza, Italy.
J Clin Oncol. 2021 Feb 20;39(6):652-662. doi: 10.1200/JCO.20.02333. Epub 2021 Jan 6.
Infant acute lymphoblastic leukemia (ALL) is characterized by a high incidence of gene rearrangements and poor outcome. We evaluated the value of minimal residual disease (MRD) in infants with -rearranged ALL treated within the Interfant-06 protocol, which compared lymphoid-style consolidation (protocol IB) versus myeloid-style consolidation (araC, daunorubicin, etoposide/mitoxantrone, araC, etoposide).
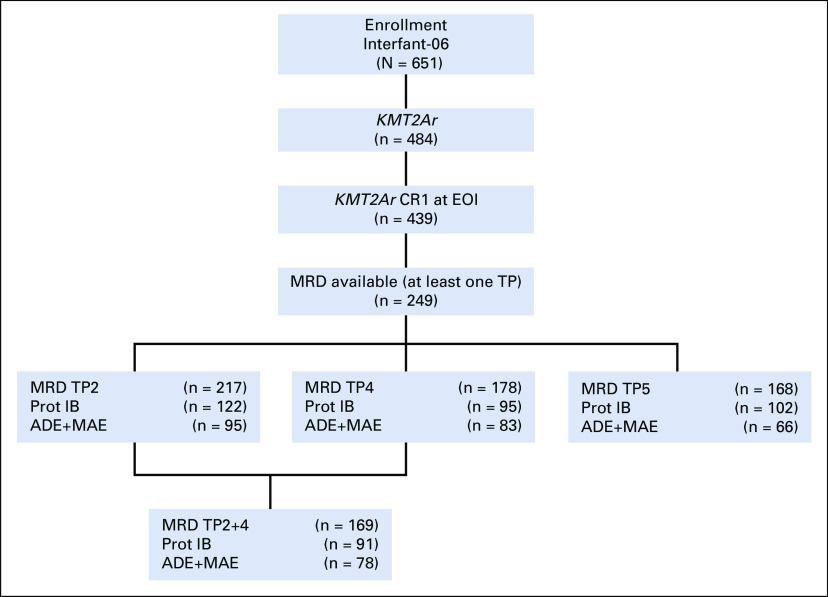
MRD was measured in 249 infants by DNA-based polymerase chain reaction of rearranged , immunoglobulin, and/or T-cell receptor genes, at the end of induction (EOI) and end of consolidation (EOC). MRD results were classified as negative, intermediate (< 5 × 10), and high (≥ 5 × 10).
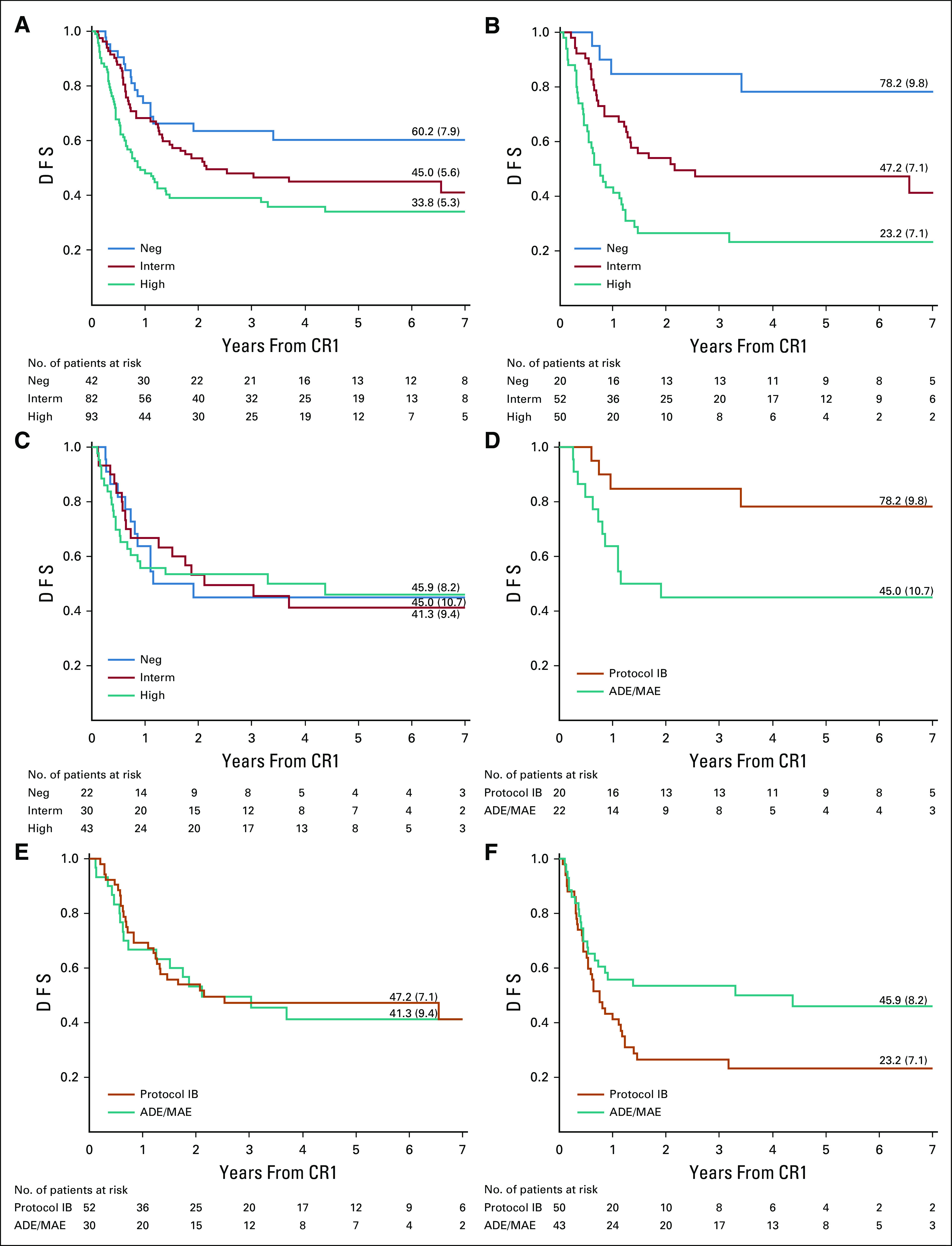
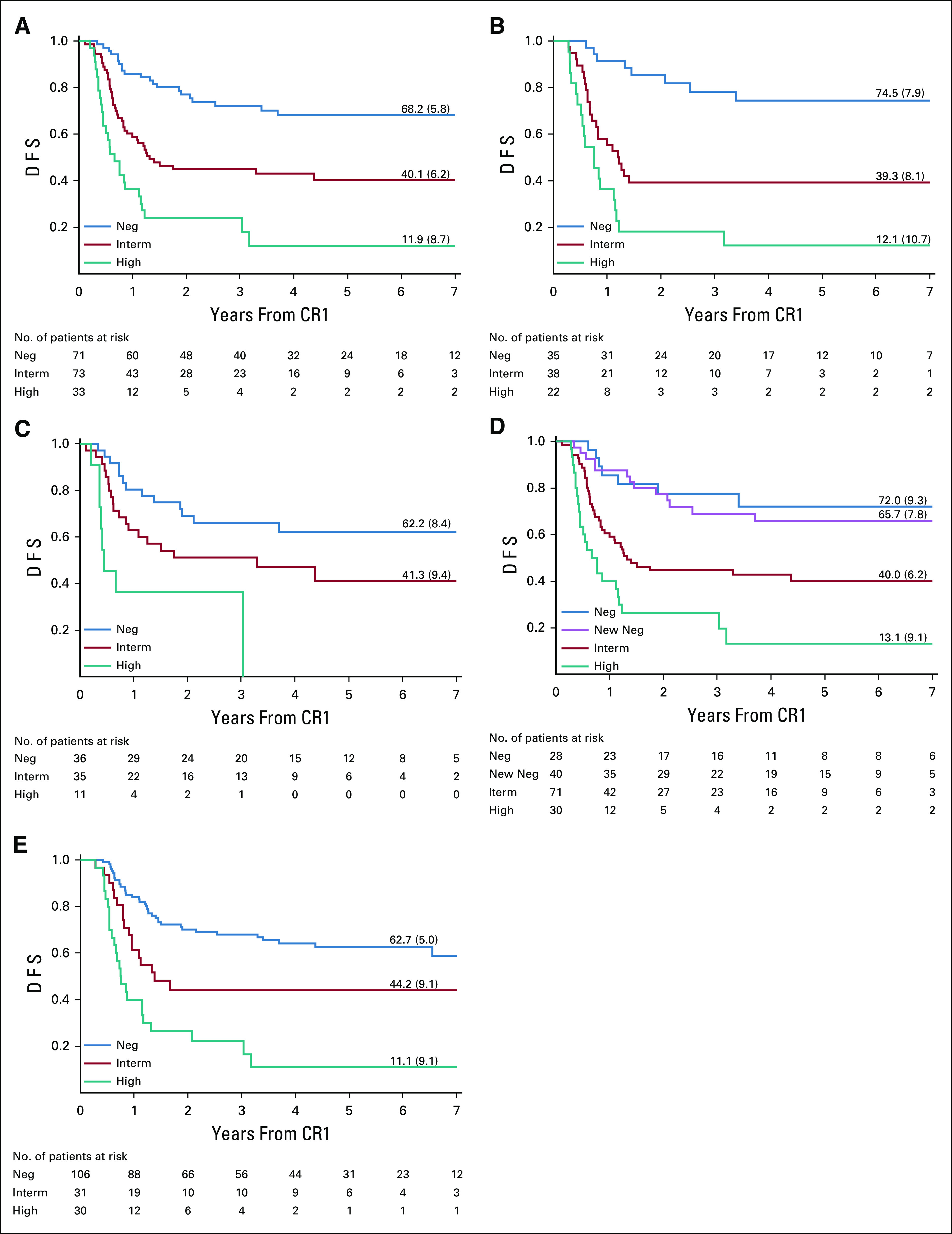
EOI MRD levels predicted outcome with 6-year disease-free survival (DFS) of 60.2% (95% CI, 43.2 to 73.6), 45.0% (95% CI, 28.3 to 53.1), and 33.8% (95% CI, 23.8 to 44.1) for infants with negative, intermediate, and high EOI MRD levels, respectively ( = .0039). EOC MRD levels were also predictive of outcome, with 6-year DFS of 68.2% (95% CI, 55.2 to 78.1), 40.1% (95% CI, 28.1 to 51.9), and 11.9% (95% CI, 2.6 to 29.1) for infants with negative, intermediate, and high EOC MRD levels, respectively ( < .0001). Analysis of EOI MRD according to the type of consolidation treatment showed that infants treated with lymphoid-style consolidation had 6-year DFS of 78.2% (95% CI, 51.4 to 91.3), 47.2% (95% CI, 33.0 to 60.1), and 23.2% (95% CI, 12.1 to 36.4) for negative, intermediate, and high MRD levels, respectively ( < .0001), while for myeloid-style-treated patients the corresponding figures were 45.0% (95% CI, 23.9 to 64.1), 41.3% (95% CI, 23.2 to 58.5), and 45.9% (95% CI, 29.4 to 60.9).
This study provides support for the idea that induction therapy selects patients for subsequent therapy; infants with high EOI MRD may benefit from AML-like consolidation (DFS 45.9% 23.2%), whereas patients with low EOI MRD may benefit from ALL-like consolidation (DFS 78.2% 45.0%). Patients with positive EOC MRD had dismal outcomes. These findings will be used for treatment interventions in the next Interfant protocol.
婴儿急性淋巴细胞白血病(ALL)的特征是基因重排发生率高,预后不良。我们评估了 - 重排 ALL 患儿在 Interfant-06 方案中接受治疗时微小残留病(MRD)的价值,该方案比较了淋巴样巩固(方案 IB)与髓样巩固(阿糖胞苷、柔红霉素、依托泊苷/米托蒽醌、阿糖胞苷、依托泊苷)。
通过基于 DNA 的聚合酶链反应,对 249 名婴儿的重排 、免疫球蛋白和/或 T 细胞受体基因在诱导结束(EOI)和巩固结束(EOC)时进行 MRD 检测。MRD 结果分为阴性、中间(<5×10)和高(≥5×10)。
EOI MRD 水平可预测预后,阴性、中间和高 EOI MRD 水平的患儿 6 年无病生存率(DFS)分别为 60.2%(95%CI,43.2 至 73.6)、45.0%(95%CI,28.3 至 53.1)和 33.8%(95%CI,23.8 至 44.1)(=0.0039)。EOC MRD 水平也可预测预后,阴性、中间和高 EOC MRD 水平的患儿 6 年 DFS 分别为 68.2%(95%CI,55.2 至 78.1)、40.1%(95%CI,28.1 至 51.9)和 11.9%(95%CI,2.6 至 29.1)(<0.0001)。根据巩固治疗类型对 EOI MRD 进行分析显示,接受淋巴样巩固治疗的患儿 6 年 DFS 分别为 78.2%(95%CI,51.4 至 91.3)、47.2%(95%CI,33.0 至 60.1)和 23.2%(95%CI,12.1 至 36.4)(<0.0001),而接受髓样巩固治疗的患儿相应数字分别为 45.0%(95%CI,23.9 至 64.1)、41.3%(95%CI,23.2 至 58.5)和 45.9%(95%CI,29.4 至 60.9)。
本研究支持诱导治疗可选择后续治疗患者的观点;EOI MRD 较高的患儿可能受益于 AML 样巩固(DFS 45.9%比 23.2%),而 EOI MRD 较低的患儿可能受益于 ALL 样巩固(DFS 78.2%比 45.0%)。EOC MRD 阳性的患儿预后不良。这些发现将用于下一个 Interfant 方案的治疗干预。