Department of Surgery, Kamuzu Central Hospital, Lilongwe, Malawi.
Department of Clinical Medicine (K1), University of Bergen, Bergen, Norway.
PLoS One. 2021 Jan 6;16(1):e0243536. doi: 10.1371/journal.pone.0243536. eCollection 2021.
There is a lack of accurate information on the prevalence and causes of musculoskeletal impairment (MSI) in low income countries. The WHO prevalence estimate does not help plan services for specific national income levels or countries. The aim of this study was to find the prevalence, impact, causes and factors associated with musculoskeletal impairment in Malawi. We wished to undertake a national cluster randomized survey of musculoskeletal impairment in Malawi, one of the UN Least Developed Countries (LDC), that involved a reliable sampling methodology with a case definition and diagnostic criteria that could clearly be related to the classification system used in the WHO International Classification of Functioning, Disability and Health (ICF).
A sample size of 1,481 households was calculated using data from the latest national census and an expected prevalence based on similar surveys conducted in Rwanda and Cameroon. We randomly selected clusters across the whole country through probability proportional to size sampling with an urban/rural and demographic split that matched the distribution of the population. In the field, randomization of households in a cluster was based on a ground bottle spin. All household members present were screened, and all MSI cases identified were examined in more detail by medical students under supervision, using a standardized interview and examination protocol. Data collection was carried out from 1st July to 30th August 2016. Extrapolation was done based on study size compared to the population of Malawi. MSI severity was classified using the parameters for the percentage of function outlined in the WHO International Classification of Functioning (ICF). A loss of function of 5-24% was mild, 25-49% was moderate and 50-90% was severe. The Malawian version of the EQ-5D-3L questionnaire was used, and EQ-5D index scores were calculated using population values from Zimbabwe, as a population value set for Malawi is not currently available. Chi-square test was used to test categorical variables. Odds ratio (OR) was calculated with a linear regression model adjusted for age, gender, location and education.
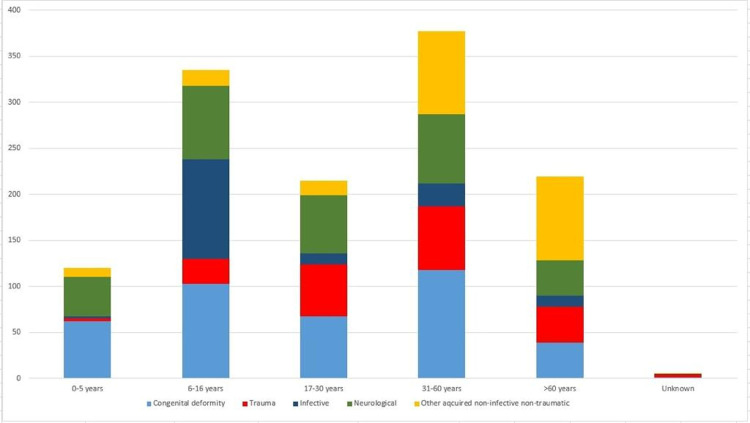
A total of 8,801 individuals were enumerated in 1,481 households. Of the 8,548 participants that were screened and examined (response rate of 97.1%), 810 cases of MSI were diagnosed of which 18% (108) had mild, 54% (329) had moderate and 28% (167) had severe MSI as classified by ICF. There was an overall prevalence of MSI of 9.5% (CI 8.9-10.1). The prevalence of MSI increased with age, and was similar in men (9.3%) and women (9.6%). People without formal education were more likely to have MSI [13.3% (CI 11.8-14.8)] compared to those with formal education levels [8.9% (CI 8.1-9.7), p<0.001] for primary school and [5.9% (4.6-7.2), p<0.001] for secondary school. Overall, 33.2% of MSIs were due to congenital causes, 25.6% were neurological in origin, 19.2% due to acquired non-traumatic non-infective causes, 16.8% due to trauma and 5.2% due to infection. Extrapolation of these findings indicated that there are approximately one million cases of MSI in Malawi that need further treatment. MSI had a profound impact on quality of life. Analysis of disaggregated quality of life measures using EQ-5D showed clear correlation with the ICF class. A large proportion of patients with moderate and severe MSI were confined to bed, unable to wash or undress or unable to perform usual daily activities.
This study has uncovered a high prevalence of MSI in Malawi and its profound impact on a large proportion of the population. These findings suggest that MSI places a considerable strain on social and financial structures in this low-income country. The Quality of Life of those with severe MSI is considerably affected. The huge burden of musculoskeletal impairment in Malawi is mostly unattended, revealing an urgent need to scale up surgical and rehabilitation services in the country.
在低收入国家,有关肌肉骨骼损伤(MSI)的流行率和病因的准确信息十分匮乏。世卫组织的流行率估计无助于针对特定国家收入水平或国家规划服务。本研究的目的是在马拉维(联合国最不发达国家之一)确定肌肉骨骼损伤的流行率、影响、病因和相关因素。我们希望对马拉维的肌肉骨骼损伤进行全国性的聚类随机调查,该调查涉及一种可靠的抽样方法,其病例定义和诊断标准可以明确与世卫组织《国际功能、残疾和健康分类》(ICF)中使用的分类系统相关联。
我们根据最新的全国人口普查数据和基于在卢旺达和喀麦隆进行的类似调查的预期流行率计算了 1481 户家庭的样本量。我们通过概率比例抽样在全国范围内随机选择集群,城乡和人口分布与人口分布相匹配。在实地,基于地面瓶旋转对集群中的家庭进行随机化。对所有在场的家庭成员进行筛查,由医学生在监督下使用标准化访谈和检查方案对所有确定的 MSI 病例进行更详细的检查。数据收集工作于 2016 年 7 月 1 日至 8 月 30 日进行。根据与马拉维人口相比的研究规模进行外推。使用世卫组织《国际功能分类(ICF)》中概述的功能百分比参数对 MSI 严重程度进行分类。功能丧失 5-24%为轻度,25-49%为中度,50-90%为重度。使用津巴布韦的 EQ-5D-3L 问卷版本,并使用人口值计算 EQ-5D 指数评分,因为目前尚无适用于马拉维的人口值集。使用卡方检验检验分类变量。使用线性回归模型调整年龄、性别、位置和教育因素计算比值比(OR)。
在 1481 户家庭中总计登记了 8801 人。在接受筛查和检查的 8548 名参与者中(应答率为 97.1%),诊断出 810 例 MSI,其中 18%(108 例)为轻度,54%(329 例)为中度,28%(167 例)为重度,根据 ICF 进行分类。总体 MSI 患病率为 9.5%(CI 8.9-10.1)。MSI 患病率随年龄增长而增加,男性(9.3%)和女性(9.6%)之间相似。未受过正规教育的人比受过正规教育的人更容易患有 MSI[13.3%(CI 11.8-14.8)]与小学(9.9%(CI 8.1-9.7),p<0.001)和中学(5.9%(4.6-7.2),p<0.001)相比。总体而言,33.2%的 MSI 是由先天性原因引起的,25.6%是神经源性的,19.2%是由后天性非创伤性非感染性原因引起的,16.8%是由创伤引起的,5.2%是由感染引起的。这些发现的外推表明,马拉维约有 100 万例 MSI 需要进一步治疗。MSI 对生活质量产生了深远的影响。使用 EQ-5D 分析离散的生活质量措施显示出与 ICF 类别明确的相关性。大量患有中度和重度 MSI 的患者卧床不起,无法洗漱或穿衣,或无法进行日常活动。
本研究揭示了马拉维肌肉骨骼损伤的高患病率及其对大部分人口的巨大影响。这些发现表明,MSI 给这个低收入国家的社会和财政结构带来了相当大的压力。严重 MSI 患者的生活质量受到了相当大的影响。马拉维肌肉骨骼损伤的巨大负担大部分未得到重视,迫切需要在该国扩大手术和康复服务。