Tsubaki Masanobu, Takeda Tomoya, Matsuda Takuya, Seki Shiori, Tomonari Yoshika, Koizumi Shoutaro, Nagatakiya Miki, Katsuyama Mai, Yamamoto Yuuta, Tsurushima Katsumasa, Ishizaka Toshihiko, Nishida Shozo
Division of Pharmacotherapy, Kindai University School of Pharmacy, Kowakae, Higashi-Osaka 577-8502, Japan.
Department of Pharmacy, Sakai City Medical Center, Sakai 593-8304, Japan.
Biomedicines. 2021 Jan 4;9(1):33. doi: 10.3390/biomedicines9010033.
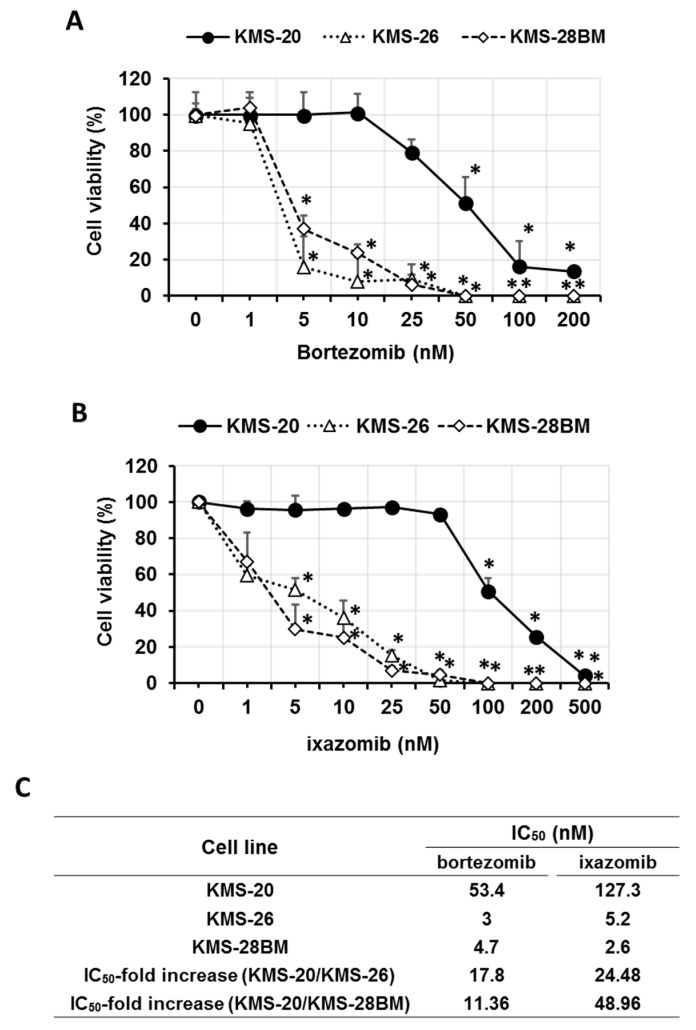
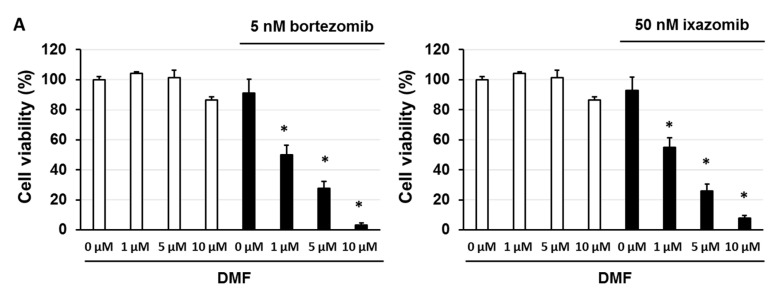
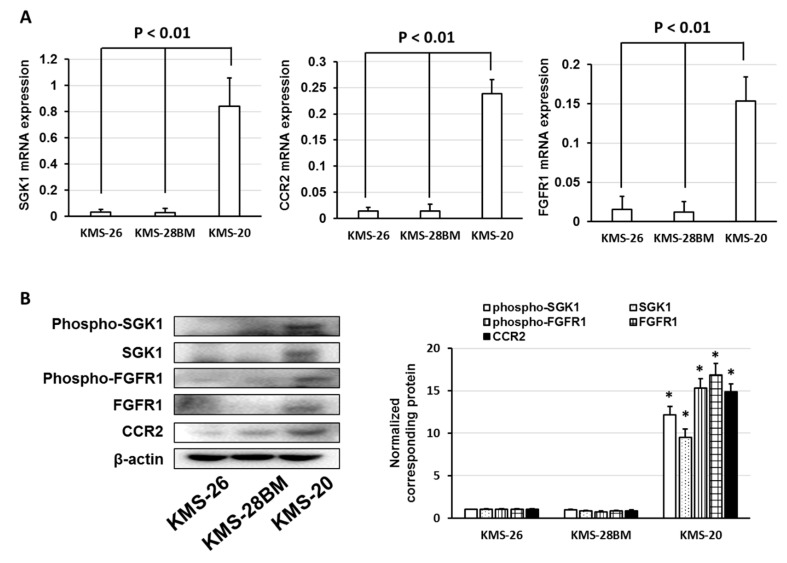
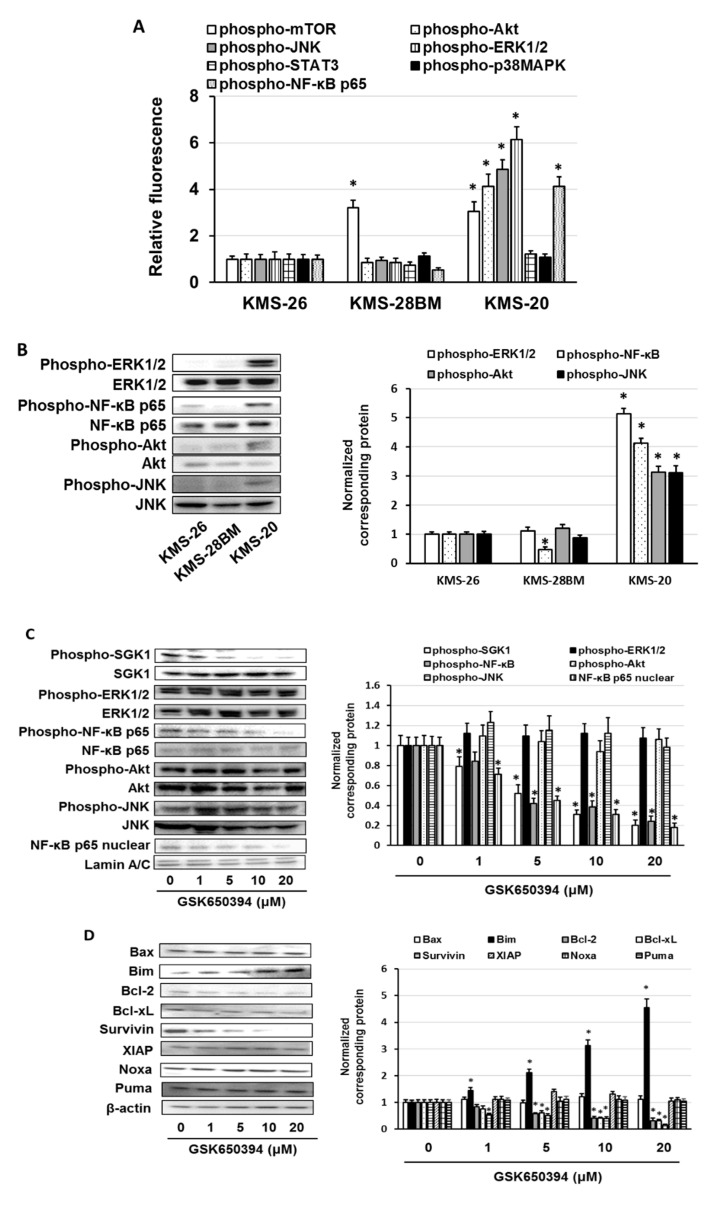
Multiple myeloma (MM) is an incurable malignancy often associated with primary and acquired resistance to therapeutic agents, such as proteasome inhibitors. However, the mechanisms underlying the proteasome inhibitor resistance are poorly understood. Here, we elucidate the mechanism of primary resistance to bortezomib and ixazomib in the MM cell lines, KMS-20, KMS-26, and KMS-28BM. We find that low bortezomib and ixazomib concentrations induce cell death in KMS-26 and KMS-28BM cells. However, high bortezomib and ixazomib concentrations induce cell death only in KMS-20 cells. During Gene Expression Omnibus analysis, KMS-20 cells exhibit high levels of expression of various genes, including , , and . The SGK1 inhibitor enhances the cytotoxic effects of bortezomib and ixazomib; however, FGFR1 and CCR2 inhibitors do not show such effect in KMS-20 cells. Moreover, SGK1 activation induces the phosphorylation of NF-κB p65, and an NF-κB inhibitor enhances the sensitivity of KMS-20 cells to bortezomib and ixazomib. Additionally, high levels of expression of SGK1 and NF-κB p65 is associated with a low sensitivity to bortezomib and a poor prognosis in MM patients. These results indicate that the activation of the SGK1/NF-κB pathway correlates with a low sensitivity to bortezomib and ixazomib, and a combination of bortezomib and ixazomib with an SGK1 or NF-κB inhibitor may be involved in the treatment of MM via activation of the SGK1/NF-κB pathway.
多发性骨髓瘤(MM)是一种无法治愈的恶性肿瘤,常与对治疗药物(如蛋白酶体抑制剂)的原发性和获得性耐药相关。然而,蛋白酶体抑制剂耐药的潜在机制尚不清楚。在此,我们阐明了MM细胞系KMS-20、KMS-26和KMS-28BM对硼替佐米和伊沙佐米原发性耐药的机制。我们发现低浓度的硼替佐米和伊沙佐米可诱导KMS-26和KMS-28BM细胞死亡。然而,高浓度的硼替佐米和伊沙佐米仅在KMS-20细胞中诱导细胞死亡。在基因表达综合分析中,KMS-20细胞表现出多种基因的高表达水平,包括 、 和 。SGK1抑制剂增强了硼替佐米和伊沙佐米的细胞毒性作用;然而,FGFR1和CCR2抑制剂在KMS-20细胞中未显示出这种作用。此外,SGK1激活诱导NF-κB p65磷酸化,NF-κB抑制剂增强KMS-20细胞对硼替佐米和伊沙佐米的敏感性。此外,SGK1和NF-κB p65的高表达水平与MM患者对硼替佐米的低敏感性和不良预后相关。这些结果表明,SGK1/NF-κB通路的激活与对硼替佐米和伊沙佐米的低敏感性相关,硼替佐米和伊沙佐米与SGK1或NF-κB抑制剂联合使用可能通过激活SGK1/NF-κB通路参与MM的治疗。