Decharatanachart Pakanat, Chaiteerakij Roongruedee, Tiyarattanachai Thodsawit, Treeprasertsuk Sombat
Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Division of Gastroenterology, Department of Medicine, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, 1873 Rama IV Rd., Pathum Wan, Bangkok, 10330, Thailand.
BMC Gastroenterol. 2021 Jan 6;21(1):10. doi: 10.1186/s12876-020-01585-5.
The gold standard for the diagnosis of liver fibrosis and nonalcoholic fatty liver disease (NAFLD) is liver biopsy. Various noninvasive modalities, e.g., ultrasonography, elastography and clinical predictive scores, have been used as alternatives to liver biopsy, with limited performance. Recently, artificial intelligence (AI) models have been developed and integrated into noninvasive diagnostic tools to improve their performance.
We systematically searched for studies on AI-assisted diagnosis of liver fibrosis and NAFLD on MEDLINE, Scopus, Web of Science and Google Scholar. The pooled sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and diagnostic odds ratio (DOR) with their 95% confidence intervals (95% CIs) were calculated using a random effects model. A summary receiver operating characteristic curve and the area under the curve was generated to determine the diagnostic accuracy of the AI-assisted system. Subgroup analyses by diagnostic modalities, population and AI classifiers were performed.
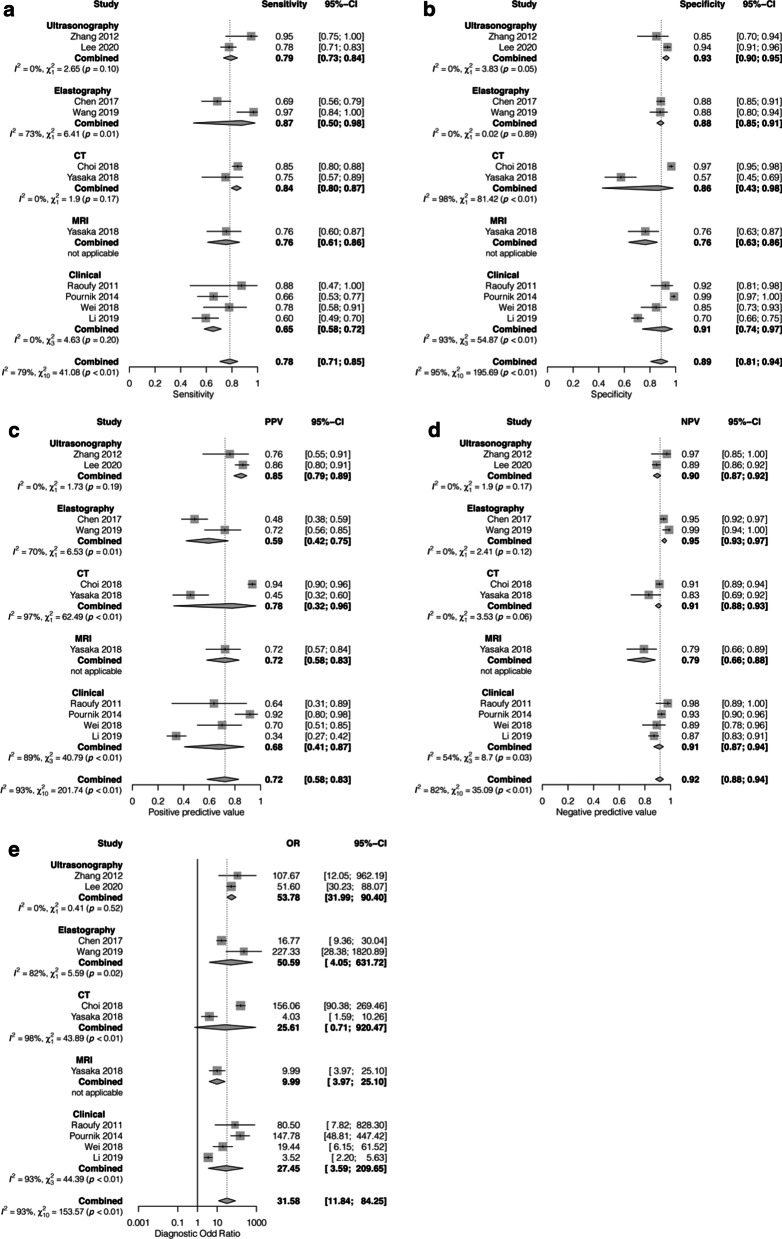
We included 19 studies reporting the performances of AI-assisted ultrasonography, elastrography, computed tomography, magnetic resonance imaging and clinical parameters for the diagnosis of liver fibrosis and steatosis. For the diagnosis of liver fibrosis, the pooled sensitivity, specificity, PPV, NPV and DOR were 0.78 (0.71-0.85), 0.89 (0.81-0.94), 0.72 (0.58-0.83), 0.92 (0.88-0.94) and 31.58 (11.84-84.25), respectively, for cirrhosis; 0.86 (0.80-0.90), 0.87 (0.80-0.92), 0.85 (0.75-0.91), 0.88 (0.82-0.92) and 37.79 (16.01-89.19), respectively; for advanced fibrosis; and 0.86 (0.78-0.92), 0.81 (0.77-0.84), 0.88 (0.80-0.93), 0.77 (0.58-0.89) and 26.79 (14.47-49.62), respectively, for significant fibrosis. Subgroup analyses showed significant differences in performance for the diagnosis of fibrosis among different modalities. The pooled sensitivity, specificity, PPV, NPV and DOR were 0.97 (0.76-1.00), 0.91 (0.78-0.97), 0.95 (0.87-0.98), 0.93 (0.80-0.98) and 191.52 (38.82-944.81), respectively, for the diagnosis of liver steatosis.
AI-assisted systems have promising potential for the diagnosis of liver fibrosis and NAFLD. Validations of their performances are warranted before implementing these AI-assisted systems in clinical practice.
The protocol was registered with PROSPERO (CRD42020183295).
肝纤维化和非酒精性脂肪性肝病(NAFLD)诊断的金标准是肝活检。各种非侵入性检查方法,如超声检查、弹性成像和临床预测评分,已被用作肝活检的替代方法,但性能有限。最近,人工智能(AI)模型已被开发并集成到非侵入性诊断工具中以提高其性能。
我们在MEDLINE、Scopus、科学网和谷歌学术上系统检索了关于AI辅助诊断肝纤维化和NAFLD的研究。使用随机效应模型计算合并敏感性、特异性、阳性预测值(PPV)、阴性预测值(NPV)和诊断比值比(DOR)及其95%置信区间(95%CI)。生成汇总受试者工作特征曲线和曲线下面积以确定AI辅助系统的诊断准确性。按诊断方法、人群和AI分类器进行亚组分析。
我们纳入了19项报告AI辅助超声检查、弹性成像、计算机断层扫描、磁共振成像和临床参数用于诊断肝纤维化和脂肪变性性能的研究。对于肝纤维化的诊断,肝硬化的合并敏感性、特异性、PPV、NPV和DOR分别为0.78(0.71 - 0.85)、0.89(0.81 - 0.94)、0.72(0.58 - 0.83)、0.92(0.88 - 0.94)和31.58(11.84 - 84.25);晚期纤维化分别为0.86(0.80 - 0.90)、0.87(0.80 - 0.92)、0.85(0.75 - 0.91)、0.88(0.82 - 0.92)和37.79(16.01 - 89.19);显著纤维化分别为0.86(0.78 - 0.92)、0.81(0.77 - 0.84)、0.88(0.80 - 0.93)、0.77(0.58 - 0.89)和26.79(14.47 - 49.62)。亚组分析显示不同方法在纤维化诊断性能上存在显著差异。对于肝脂肪变性的诊断,合并敏感性、特异性、PPV、NPV和DOR分别为0.97(0.76 - 1.00)、0.91(0.78 - 0.97)、0.95(0.87 - 0.98)、0.93(0.80 - 0.98)和191.52(38.82 - 944.81)。
AI辅助系统在肝纤维化和NAFLD诊断方面具有广阔前景。在临床实践中应用这些AI辅助系统之前,有必要对其性能进行验证。
该方案已在国际前瞻性系统评价注册库(PROSPERO)注册(CRD42020183295)。