Department of Neurosurgery, Kantonsspital Aarau, Tellstrasse, 5001, Aarau, Switzerland.
Department of Health Sciences and Technology, ETH Zurich, Zurich, Switzerland.
BMC Surg. 2021 Jan 6;21(1):19. doi: 10.1186/s12893-020-01011-3.
An annular closure device (ACD) could potentially prevent recurrent herniation by blocking larger annular defects after limited microdiscectomy (LMD). The purpose of this study was to analyze the incidence of endplate changes (EPC) and outcome after LMD with additional implantation of an ACD to prevent reherniation.
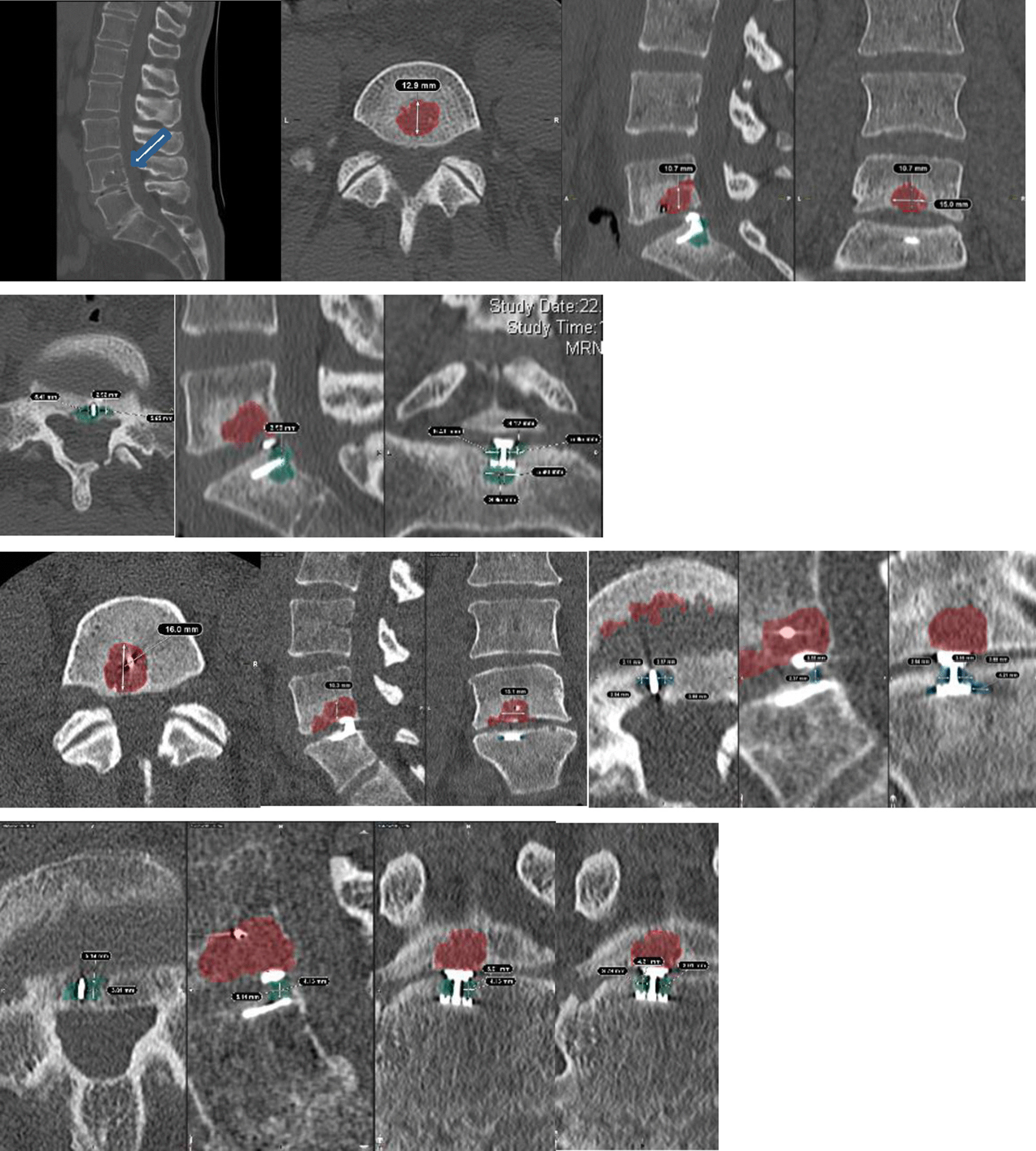
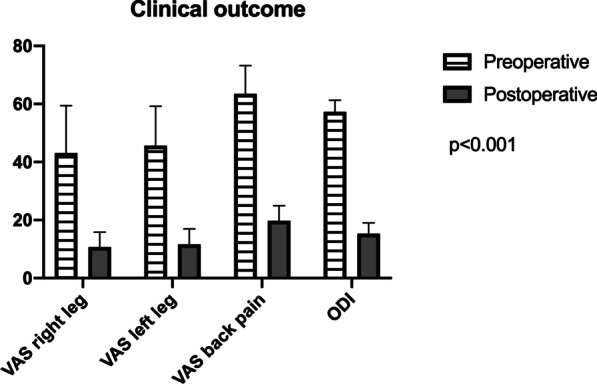
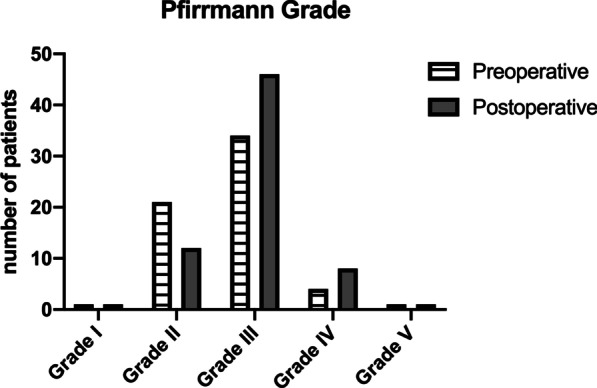
This analysis includes data from a) RCT study-arm of patients undergoing LMD with ACD implantation and b) additional patients undergoing ACD implantation at our institution. Clinical findings (VAS, ODI), radiological outcome (reherniation, implant integrity, volume of EPC) and risk factors for EPC were assessed.
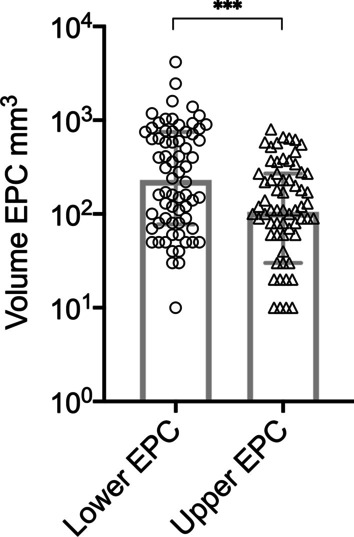
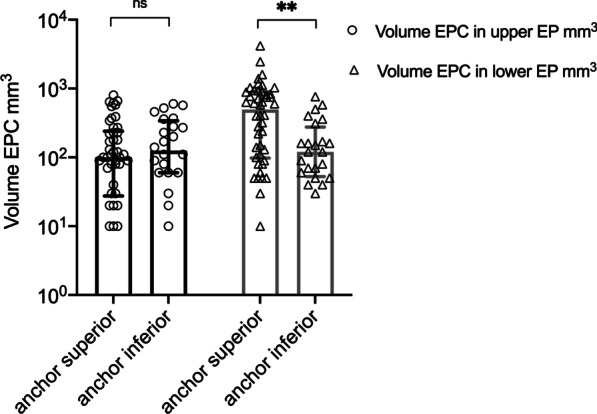
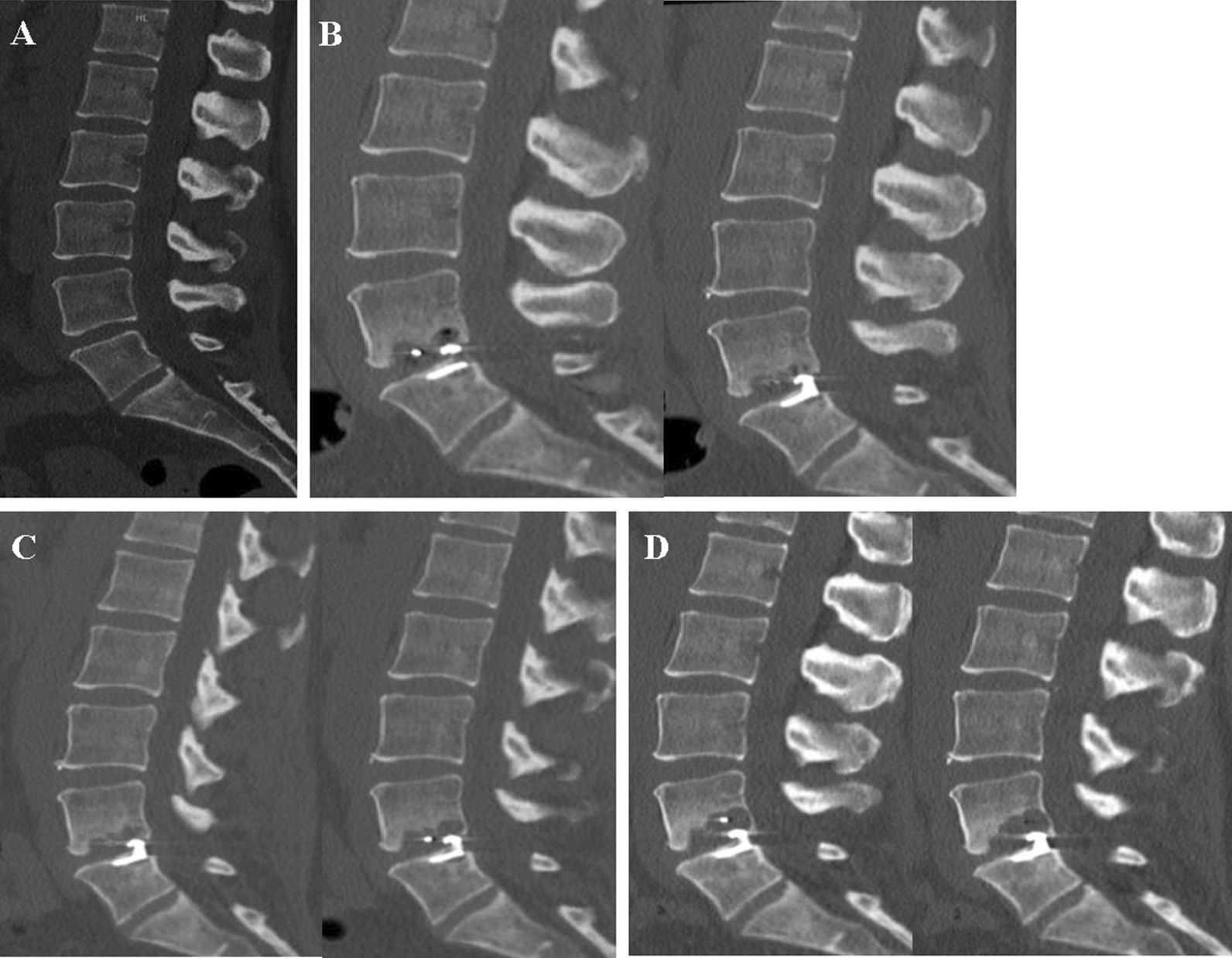
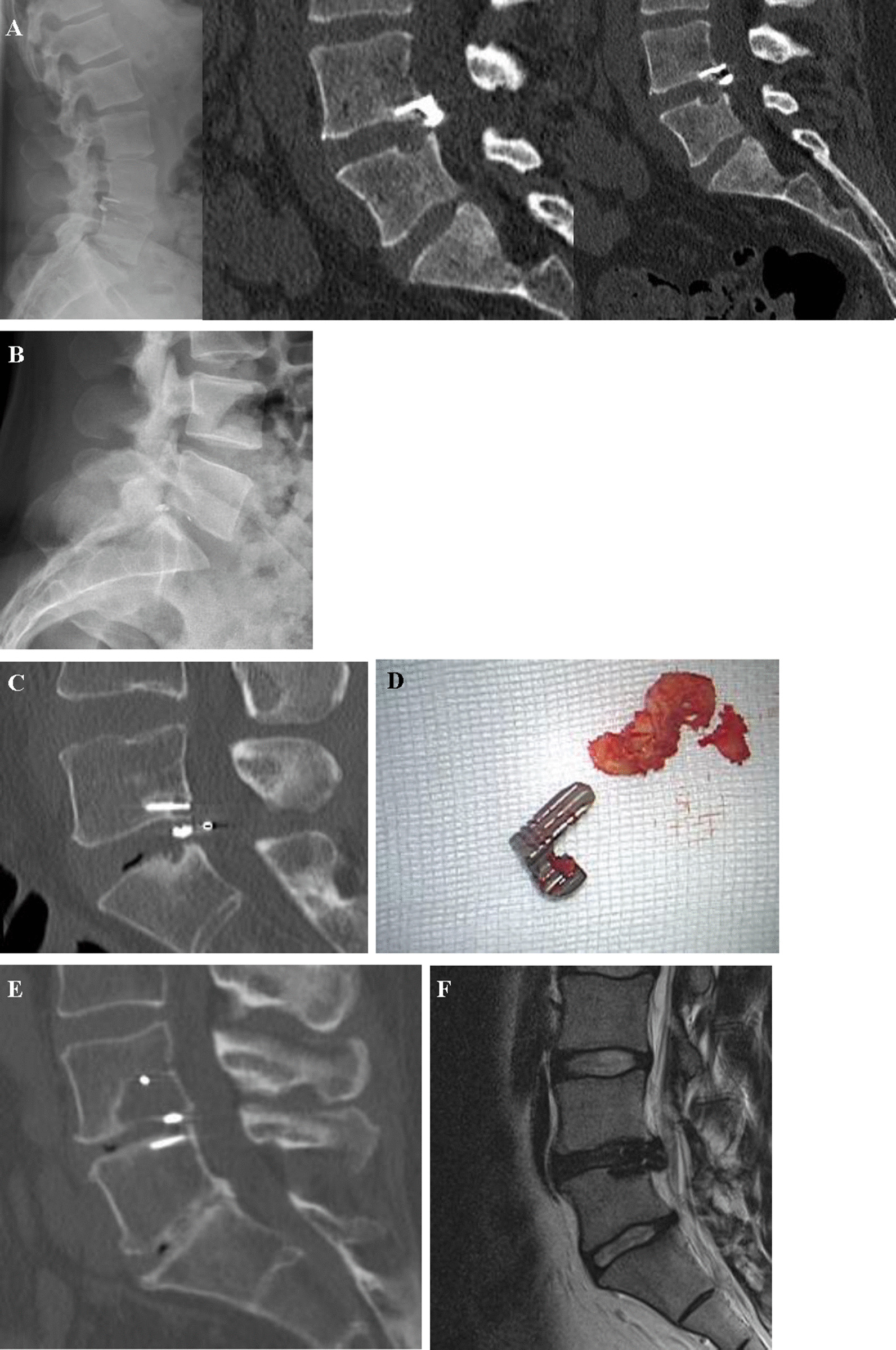
Seventy-two patients (37 men, 47 ± 11.63yo) underwent LMD and ACD implantation between 2013-2016. A total of 71 (99%) patients presented with some degree of EPC during the follow-up period (14.67 ± 4.77 months). In the multivariate regression analysis, localization of the anchor was the only significant predictor of EPC (p = 0.038). The largest EPC measured 4.2 cm. Reherniation was documented in 17 (24%) patients (symptomatic: n = 10; asymptomatic: n = 7). Six (8.3%) patients with symptomatic reherniation underwent rediscectomy. Implant failure was documented in 19 (26.4%) patients including anchor head breakage (n = 1, 1.3%), dislocation of the whole device (n = 5, 6.9%), and mesh dislocation into the spinal canal (n = 13, 18%). Mesh subsidence within the EPC was documented in 15 (20.8%) patients. Seven (9.7%) patients underwent explantation of the entire, or parts of the device.
Clinical improvement after LMD and ACD implantation was proven in our study. High incidence and volume of EPC did not correlate with clinical outcome. The ACD might prevent disc reherniation despite implant failure rates. Mechanical friction of the polymer mesh with the endplate is most likely the cause of EPC after ACD.
环形闭合装置(ACD)可通过在有限的显微减压(LMD)后阻止较大的环形缺陷,从而防止复发性疝。本研究的目的是分析在 LMD 中额外植入 ACD 以防止再疝后终板变化(EPC)的发生率和结果。
本分析包括 a)接受 LMD 联合 ACD 植入的 RCT 研究臂患者的数据,和 b)在我们机构接受 ACD 植入的额外患者的数据。评估临床发现(VAS、ODI)、放射学结果(再疝、植入物完整性、EPC 体积)和 EPC 的危险因素。
72 例患者(37 例男性,47±11.63 岁)于 2013-2016 年接受 LMD 和 ACD 植入。在整个随访期间,71(99%)例患者出现不同程度的 EPC(14.67±4.77 个月)。在多变量回归分析中,锚定位置是 EPC 的唯一显著预测因素(p=0.038)。最大的 EPC 测量值为 4.2cm。17 例(24%)患者出现疝复发(症状性:n=10;无症状性:n=7)。6 例(8.3%)症状性疝复发患者接受了再椎间盘切除术。19 例(26.4%)患者出现植入物失败,包括锚头断裂(n=1,1.3%)、整个装置脱位(n=5,6.9%)和网片向椎管内移位(n=13,18%)。15 例(20.8%)患者的网片下陷至 EPC 内。7 例(9.7%)患者行全部或部分装置取出术。
本研究证实了 LMD 和 ACD 植入后的临床改善。高发生率和大量 EPC 与临床结果无关。尽管植入物失败率较高,但 ACD 仍可防止椎间盘再疝。聚合物网片与终板之间的机械摩擦可能是 ACD 后 EPC 的原因。