Department of Rheumatology, Capital Institute of Pediatrics-Peking University Teaching Hospital, 2 Yabao Road, Beijing, China.
Department of Cardiology, Capital Institute of Pediatrics-Peking University Teaching Hospital, 2 Yabao Road, Beijing, China.
Pediatr Rheumatol Online J. 2021 Jan 6;19(1):2. doi: 10.1186/s12969-020-00486-x.
To summarize the characteristics of gastrointestinal (GI) perforation in anti-nuclear matrix protein 2 (NXP2) antibody-associated juvenile dermatomyositis (JDM).
Five patients with GI perforation from a JDM cohort of 120 cases are described. Relevant literature was reviewed.
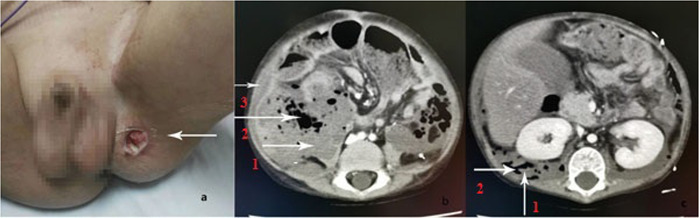
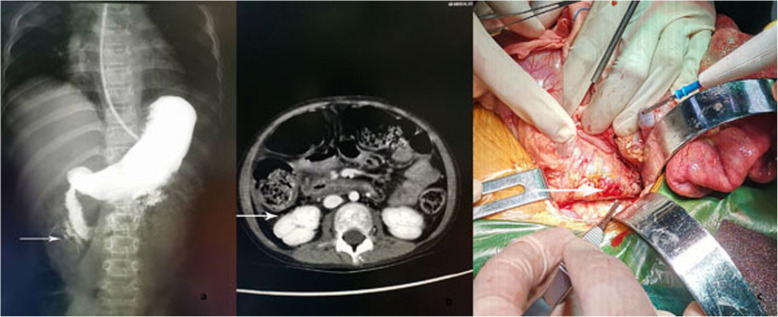
Five patients, including four females and one male, were included in the study. The age of onset of these patients ranged from 3.3 to 9.5 years with the median age of 5.0 years. When these patients were complicated by GI perforation, childhood myositis assessment score (CMAS) ranged from 1 to 5 with the median score of 2. Myositis-specific antibody (MSA) spectrum analysis indicated that the five patients were anti-NXP2 antibody positive. The initial symptoms of GI perforation were progressive abdominal pain and intermittent fever. Two patients also presented with ureteral calculus with hydronephrosis and ureteral stricture. Surgery was performed in four patients. One patient failed to undergo a repair as the perforation was high in position. For the other three patients, perforation repair was successful, of which two patients failed due to recurrent perforation. At 24 months postoperative follow-up, one patient was in complete remission on prednisone (Pred) and methotrexate (MTX) treatment, and her ureteral stricture had disappeared. The other four patients died. Adding these cases with 16 other patients described in the literature, the symptom at onset was progressive abdominal pain, which often occurred within 10 months after JDM was diagnosed. Perforation most commonly occurred in the duodenum, although it also occurred at multiple sites or was recurrent. The mortality rate of GI perforation in JDM was 38% (8/21).
All the five perforation cases in our study subjected to MSA analysis were anti-NXP2 antibody positive. The symptom at onset was abdominal pain. The most common site of perforation was the duodenum in the retroperitoneum, and the lack of acute abdominal manifestations prevented early diagnosis. GI perforation may be a fatal complication in JDM, and early diagnosis is very important. More research is needed to determine the pathogenesis and predictive factors of GI perforation in JDM.
总结抗核基质蛋白 2(NXP2)抗体相关幼年特发性皮肌炎(JDM)患者胃肠道(GI)穿孔的特征。
描述了 120 例 JDM 患者中 5 例 GI 穿孔患者的情况。回顾了相关文献。
本研究纳入了 5 例患者,其中 4 例为女性,1 例为男性,年龄 3.3-9.5 岁,中位年龄 5.0 岁。当这些患者并发 GI 穿孔时,儿童肌炎评估评分(CMAS)为 1-5 分,中位数为 2 分。肌炎特异性抗体(MSA)谱分析表明,5 例患者均为抗 NXP2 抗体阳性。GI 穿孔的初始症状为进行性腹痛和间歇性发热。2 例患者还伴有输尿管结石、肾积水和输尿管狭窄。4 例患者接受了手术。1 例因穿孔位置较高未能进行修复。对于另外 3 例患者,穿孔修复成功,但其中 2 例因再次穿孔而失败。术后 24 个月随访时,1 例患者泼尼松(Pred)和甲氨蝶呤(MTX)治疗完全缓解,其输尿管狭窄已消失。其他 4 例患者死亡。将这些病例与文献中描述的另外 16 例患者相加,起病时的症状为进行性腹痛,常在 JDM 诊断后 10 个月内发生。穿孔最常发生在十二指肠,但也可发生在多个部位或复发。JDM 患者 GI 穿孔的死亡率为 38%(8/21)。
我们研究中的所有 5 例穿孔病例均经 MSA 分析为抗 NXP2 抗体阳性。起病时的症状为腹痛。最常见的穿孔部位是腹膜后十二指肠,缺乏急性腹痛表现,导致早期诊断困难。GI 穿孔可能是 JDM 的致命并发症,早期诊断非常重要。需要进一步研究以确定 JDM 患者 GI 穿孔的发病机制和预测因素。