Imperial Centre for Endocrinology, Imperial College Healthcare NHS Trust, London, UK.
Department of Metabolism, Digestion and Reproduction, Imperial College London, London, UK.
BMJ Open Diabetes Res Care. 2021 Jan;9(1). doi: 10.1136/bmjdrc-2020-001858.
Patients with diabetes mellitus admitted to hospital with COVID-19 have poorer outcomes. However, the drivers of poorer outcomes are not fully elucidated. We performed detailed characterization of patients with COVID-19 to determine the clinical and biochemical factors that may be drivers of poorer outcomes.
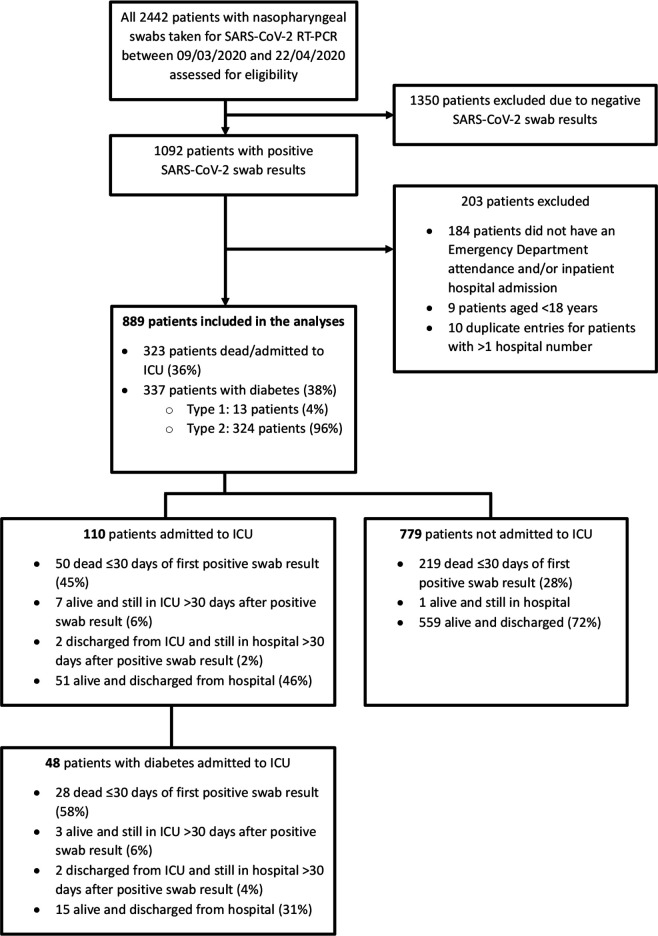
This is a retrospective cohort study of 889 consecutive inpatients diagnosed with COVID-19 between March 9 and April 22, 2020 in a large London National Health Service Trust. Unbiased multivariate logistic regression analysis was performed to determine variables that were independently and significantly associated with increased risk of death and/or intensive care unit (ICU) admission within 30 days of COVID-19 diagnosis.
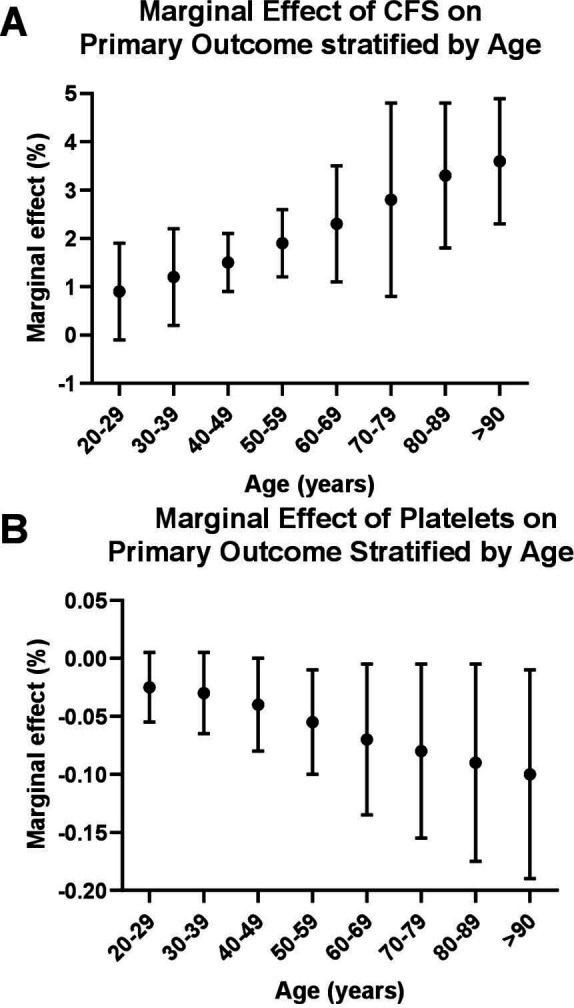
62% of patients in our cohort were of non-white ethnic background and the prevalence of diabetes was 38%. 323 (36%) patients met the primary outcome of death/admission to the ICU within 30 days of COVID-19 diagnosis. Male gender, lower platelet count, advancing age and higher Clinical Frailty Scale (CFS) score (but not diabetes) independently predicted poor outcomes on multivariate analysis. Antiplatelet medication was associated with a lower risk of death/ICU admission. Factors that were significantly and independently associated with poorer outcomes in patients with diabetes were coexisting ischemic heart disease, increasing age and lower platelet count.
In this large study of a diverse patient population, comorbidity (ie, diabetes with ischemic heart disease; increasing CFS score in older patients) was a major determinant of poor outcomes with COVID-19. Antiplatelet medication should be evaluated in randomized clinical trials among high-risk patient groups.
因 COVID-19 住院的糖尿病患者预后较差。然而,导致不良预后的原因尚未完全阐明。我们对 COVID-19 患者进行了详细的特征描述,以确定可能导致不良预后的临床和生化因素。
这是一项对 2020 年 3 月 9 日至 4 月 22 日期间在伦敦一家大型国民保健服务信托医院连续收治的 889 例 COVID-19 住院患者的回顾性队列研究。采用无偏多元逻辑回归分析确定与 COVID-19 诊断后 30 天内死亡和/或入住重症监护病房(ICU)风险增加独立且显著相关的变量。
我们队列中的 62%患者为非白人,糖尿病患病率为 38%。323 例(36%)患者在 COVID-19 诊断后 30 天内达到主要结局(死亡/入住 ICU)。男性、较低的血小板计数、年龄增长和较高的临床虚弱量表(CFS)评分(但无糖尿病)在多变量分析中独立预测不良结局。抗血小板药物与死亡/入住 ICU 的风险降低相关。与糖尿病患者预后较差显著相关的独立因素包括并存的缺血性心脏病、年龄增长和血小板计数降低。
在这项针对多种族患者人群的大型研究中,合并症(即糖尿病合并缺血性心脏病;老年患者的 CFS 评分增加)是 COVID-19 不良预后的主要决定因素。应在高危患者群体中进行抗血小板药物的随机临床试验评估。