Blizard Institute, Queen Mary University of London, London, UK, E1 2AT.
Sexual Health and HIV Medicine, Barts Health NHS Trust, London, UK, E1 1FR.
BMJ Open. 2021 Jan 17;11(1):e042140. doi: 10.1136/bmjopen-2020-042140.
To describe outcomes within different ethnic groups of a cohort of hospitalised patients with confirmed COVID-19 infection. To quantify and describe the impact of a number of prognostic factors, including frailty and inflammatory markers.
Five acute National Health Service Hospitals in east London.
Prospectively defined observational study using registry data.
1737 patients aged 16 years or over admitted to hospital with confirmed COVID-19 infection between 1 January and 13 May 2020.
The primary outcome was 30-day mortality from time of first hospital admission with COVID-19 diagnosis during or prior to admission. Secondary outcomes were 90-day mortality, intensive care unit (ICU) admission, ICU and hospital length of stay and type and duration of organ support. Multivariable survival analyses were adjusted for potential confounders.
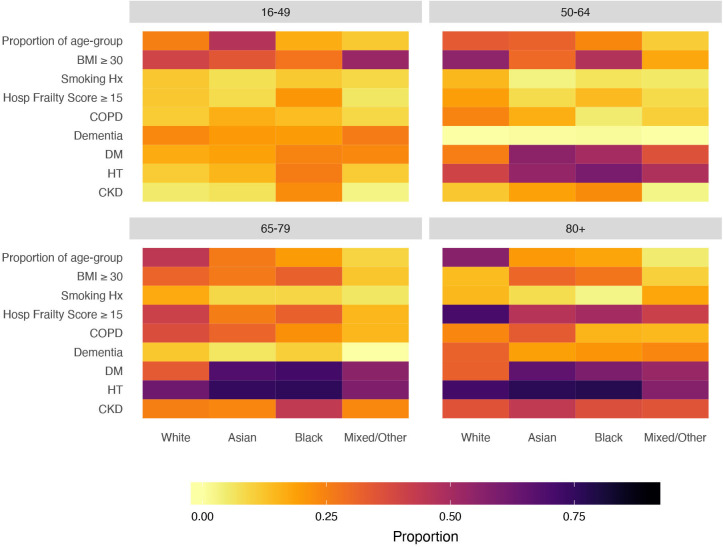
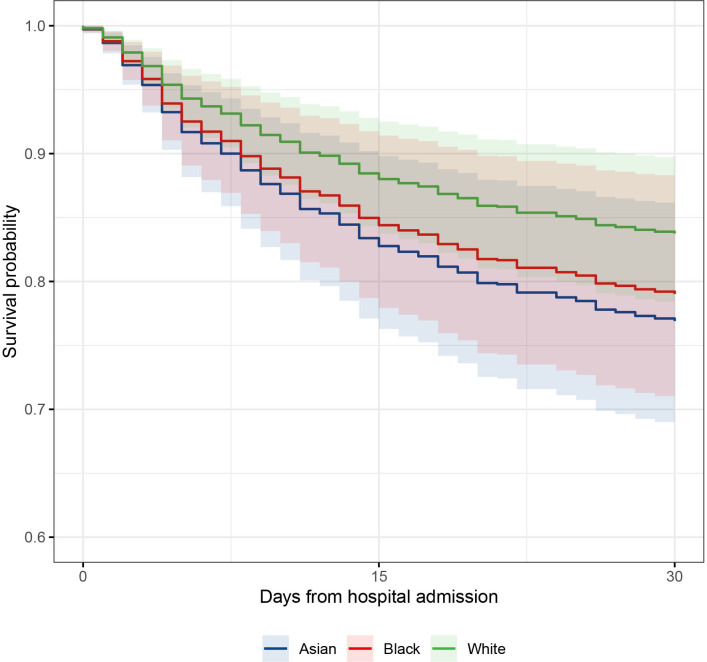
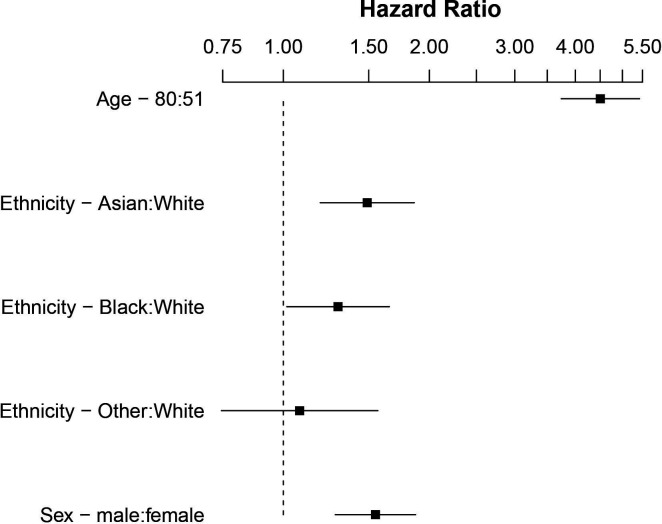
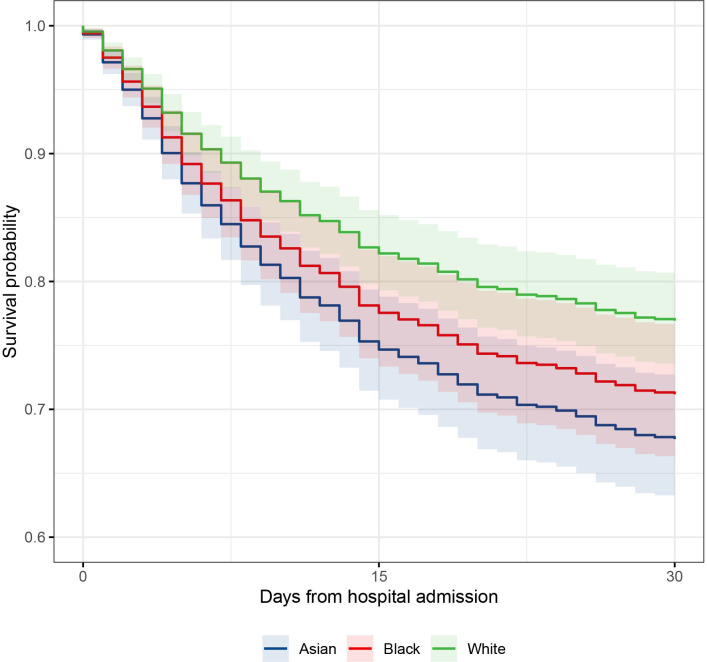
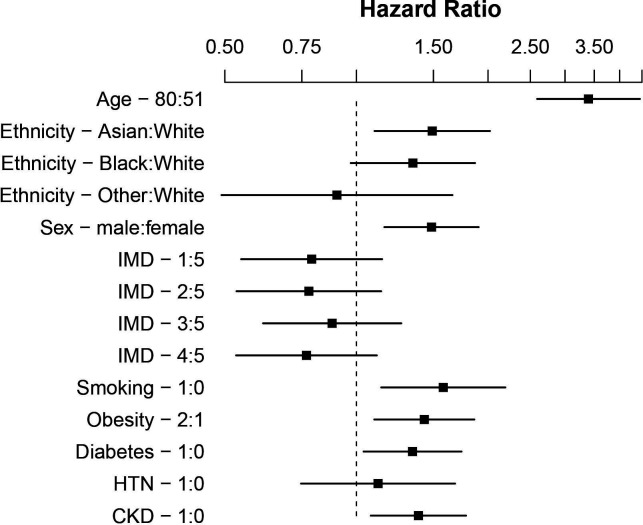
1737 were included in our analysis of whom 511 had died by day 30 (29%). 538 (31%) were from Asian, 340 (20%) black and 707 (40%) white backgrounds. Compared with white patients, those from minority ethnic backgrounds were younger, with differing comorbidity profiles and less frailty. Asian and black patients were more likely to be admitted to ICU and to receive invasive ventilation (OR 1.54, (95% CI 1.06 to 2.23); p=0.023 and OR 1.80 (95% CI 1.20 to 2.71); p=0.005, respectively). After adjustment for age and sex, patients from Asian (HR 1.49 (95% CI 1.19 to 1.86); p<0.001) and black (HR 1.30 (95% CI 1.02 to 1.65); p=0.036) backgrounds were more likely to die. These findings persisted across a range of risk factor-adjusted analyses accounting for major comorbidities, obesity, smoking, frailty and ABO blood group.
Patients from Asian and black backgrounds had higher mortality from COVID-19 infection despite controlling for all previously identified confounders and frailty. Higher rates of invasive ventilation indicate greater acute disease severity. Our analyses suggest that patients of Asian and black backgrounds suffered disproportionate rates of premature death from COVID-19.
描述确诊 COVID-19 感染住院患者的不同种族群体的结局。量化并描述包括脆弱性和炎症标志物在内的多种预后因素的影响。
东伦敦五家急性国民保健服务医院。
前瞻性定义的观察性研究,使用登记数据。
2020 年 1 月 1 日至 5 月 13 日期间,年龄在 16 岁及以上因确诊 COVID-19 感染而住院的 1737 名患者。
主要结局为从首次因 COVID-19 诊断入院至入院前或入院时 30 天的死亡率。次要结局为 90 天死亡率、重症监护病房(ICU)入院、ICU 和医院住院时间以及器官支持的类型和持续时间。多变量生存分析调整了潜在混杂因素。
我们分析了 1737 例患者,其中 511 例在第 30 天(29%)死亡。538 例(31%)来自亚洲,340 例(20%)来自黑人,707 例(40%)来自白人背景。与白人患者相比,少数民族背景的患者年龄更小,合并症谱不同,脆弱性更低。亚洲和黑人患者更有可能入住 ICU 和接受有创通气(比值比 1.54,95%置信区间 1.06 至 2.23;p=0.023 和比值比 1.80,95%置信区间 1.20 至 2.71;p=0.005)。在校正年龄和性别后,来自亚洲(风险比 1.49,95%置信区间 1.19 至 1.86;p<0.001)和黑人(风险比 1.30,95%置信区间 1.02 至 1.65;p=0.036)背景的患者更有可能死亡。这些发现在一系列考虑主要合并症、肥胖、吸烟、脆弱性和 ABO 血型的风险因素调整分析中仍然存在。
尽管控制了所有先前确定的混杂因素和脆弱性,来自亚洲和黑人背景的患者 COVID-19 感染的死亡率仍然较高。更高的有创通气率表明急性疾病严重程度更高。我们的分析表明,亚洲和黑人背景的患者 COVID-19 过早死亡的比例不成比例。