Arthur Lauren E, McMann Ashley H, Slattery Lauren N, Fuhrman George M, Mackey Aimee M, Rivere Amy E, Corsetti Ralph L
The University of Queensland Faculty of Medicine, Ochsner Clinical School, New Orleans, LA.
Department of Surgery, Lieselotte Tansey Breast Center, Ochsner Clinic Foundation, New Orleans, LA.
Ochsner J. 2020 Winter;20(4):381-387. doi: 10.31486/toj.20.0035.
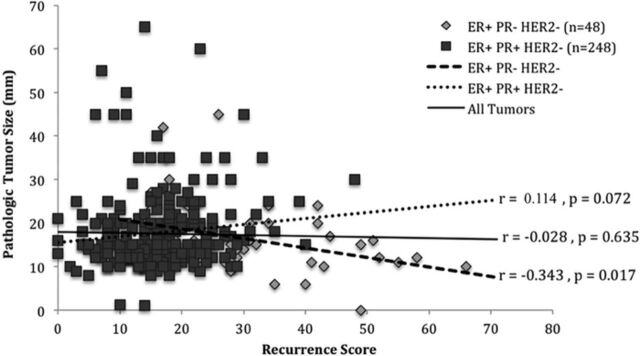
Traditionally, breast cancer is staged using TNM criteria: tumor size (T), nodal status (N), and metastasis (M). The Oncotype DX assay provides a recurrence score (RS) based on genomics that predicts the likelihood of distant recurrence in estrogen receptor-positive (ER+)/human epidermal growth factor receptor 2-negative (HER2-)/lymph node-negative (LN-) tumors. We retrospectively reviewed the medical records of patients with ER+/HER2-/LN- breast cancer tumors who were evaluated between 2007 and 2017 with Oncotype DX RS. We compared the RS to tumor size, patient age, progesterone receptor (PR) status, and LN immunohistochemistry to assess for factors that may independently predict recurrence risk. We also compared tumor size to tumor grade. The data set included 296 tumors: 248 ER+/PR-positive (PR+)/HER2- and 48 ER+/PR-negative (PR-)/HER2-. RS ranged from 0 to 66, patient age ranged from 33 to 77 years, and tumor size ranged from 1 to 65 mm. No significant correlation was found between age and RS (=-0.073, =0.208). PR- tumors had a significantly higher RS regardless of size (PR- mean RS 30.8 ± 12.7; PR+ mean RS 16.3 7.3; (53)=7.6, <0.0001). No significant correlation was seen between tumor size and RS for all tumors (=-0.028, =0.635), and this finding remained true for the PR+ tumor subgroup (=0.114, =0.072). However, a significant negative correlation was seen between tumor size and RS in the PR- subgroup (=-0.343, =0.017). Further analysis to ensure that differences in tumor grade did not account for this correlation showed equal distribution of well differentiated, moderately differentiated, and poorly differentiated tumors with no significant correlation between tumor size and grade. Increasing tumor size may not be associated with increasing biological aggressiveness. Traditionally, smaller tumors are thought to be lower risk and larger tumors higher risk, with a tendency to use chemotherapy with large tumors. However, our data showed a negative correlation between tumor size and RS in the PR- subgroup. A tumor with PR negativity that reaches a large size without metastasizing may suggest a favorable tumor biology. These tumors may not receive as much benefit from chemotherapy as previously thought. Also, the higher RS seen in smaller PR- tumors may demonstrate PR- status as a predictor for higher risk of distant recurrence. We propose that all tumors meeting the ER+/PR-/LN- criteria, regardless of size, should be considered for genotyping, with the RS used to guide chemotherapy benefit.
传统上,乳腺癌采用TNM标准进行分期:肿瘤大小(T)、淋巴结状态(N)和转移情况(M)。Oncotype DX检测基于基因组学提供一个复发评分(RS),用于预测雌激素受体阳性(ER+)/人表皮生长因子受体2阴性(HER2-)/淋巴结阴性(LN-)肿瘤远处复发的可能性。我们回顾性分析了2007年至2017年间接受Oncotype DX RS评估的ER+/HER2-/LN-乳腺癌肿瘤患者的病历。我们将RS与肿瘤大小、患者年龄、孕激素受体(PR)状态以及LN免疫组化结果进行比较,以评估可能独立预测复发风险的因素。我们还比较了肿瘤大小与肿瘤分级。数据集包括296个肿瘤:248个ER+/PR阳性(PR+)/HER2-肿瘤和48个ER+/PR阴性(PR-)/HER2-肿瘤。RS范围为0至66,患者年龄范围为33至77岁,肿瘤大小范围为1至65毫米。未发现年龄与RS之间存在显著相关性(r=-0.073,P=0.208)。无论肿瘤大小如何,PR-肿瘤的RS均显著更高(PR-组平均RS为30.8±12.7;PR+组平均RS为16.3±7.3;t(53)=7.6,P<0.0001)。所有肿瘤的肿瘤大小与RS之间均未发现显著相关性(r=-0.028,P=0.635),PR+肿瘤亚组亦是如此(r=0.114,P=0.072)。然而,PR-亚组的肿瘤大小与RS之间存在显著负相关(r=-0.343,P=0.017)。进一步分析以确保肿瘤分级差异不会导致这种相关性,结果显示高分化、中分化和低分化肿瘤分布均匀,肿瘤大小与分级之间无显著相关性。肿瘤大小增加可能与生物学侵袭性增加无关。传统上,较小的肿瘤被认为风险较低,较大的肿瘤风险较高,因此倾向于对较大肿瘤使用化疗。然而,我们的数据显示PR-亚组中肿瘤大小与RS之间存在负相关。一个PR阴性且未发生转移但体积较大的肿瘤可能提示其具有良好的肿瘤生物学特性。这些肿瘤可能无法从化疗中获得如之前认为的那么多益处。此外,较小的PR-肿瘤中较高的RS可能表明PR-状态是远处复发高风险的一个预测指标。我们建议,所有符合ER+/PR-/LN-标准的肿瘤,无论大小,均应考虑进行基因分型,使用RS来指导化疗获益。