Arfaras-Melainis Angelos, Cordero Hernando, Goyal Aditya, Benes Linda, Salgunan Reka
Internal Medicine, Albert Einstein College of Medicine, Jacobi Medical Center, Bronx, USA.
Cardiology, Attikon University Hospital, Athens, GRC.
Cureus. 2020 Nov 30;12(11):e11799. doi: 10.7759/cureus.11799.
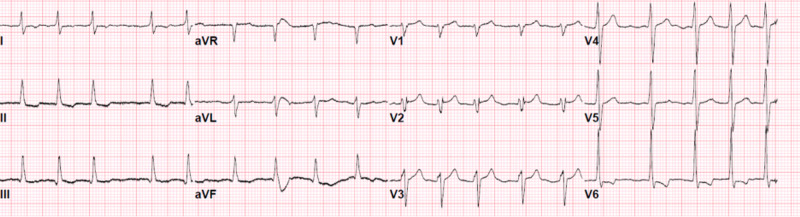
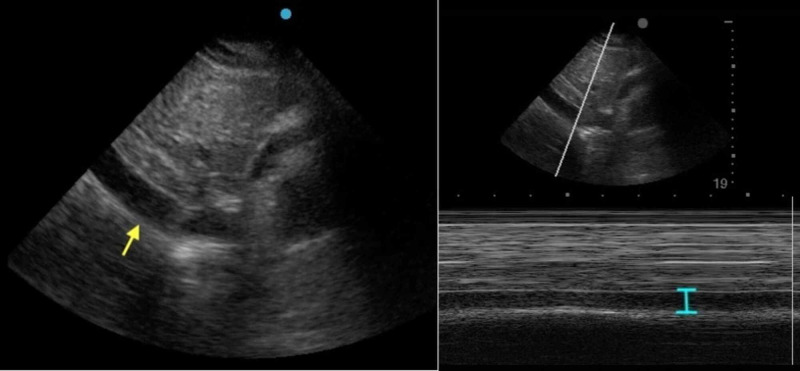
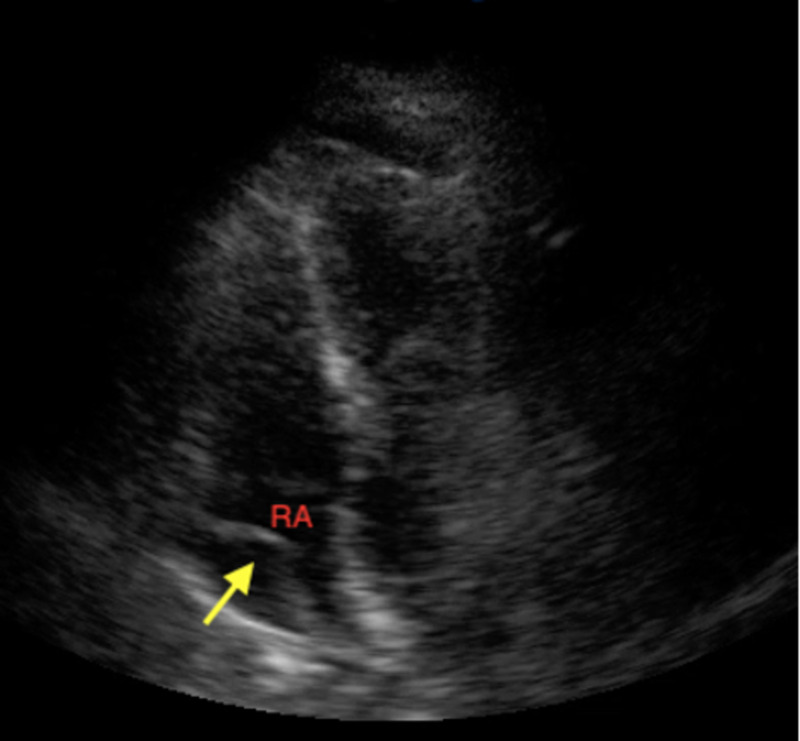
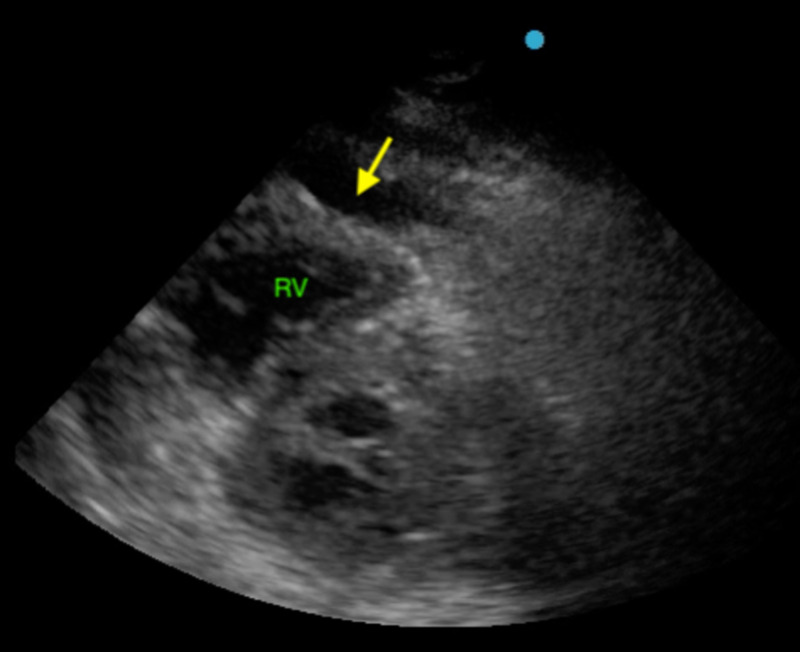
Influenza A and B acute infections usually affect primarily the respiratory system. In rare cases, however, the cardiovascular system is also compromised either via the direct effect of the virus or via the worsening of preexisting cardiac conditions. We present a rare case of acute Influenza B infection presenting as pericardial effusion and cardiac tamponade. A healthy 32-year-old female was presented to the emergency room with influenza-like symptoms for four days, where she was monitored for a few hours and was subsequently discharged to home after testing positive for Influenza B by polymerase chain reaction (PCR). On the fifth day, she returned to the emergency room with worsening symptoms, primarily exertional dyspnea. She was hypotensive and tachycardic and temporarily improved with fluid administration. She was transferred to the intensive care unit, where a bedside point of care ultrasound (POCUS) and later a formal transthoracic echocardiogram revealed that she had pericardial effusion with sonographic signs of cardiac tamponade. Emergent pericardiocentesis was performed and resulted in hemodynamic and symptomatic improvement. The pericardial drain that was initially left in place and continued to drain pericardial fluid (700 ccs in total), was removed 3 days later, after echocardiographic confirmation of the resolution of the pericardial effusion. She completed a five-day course of Oseltamivir and was subsequently discharged home safely. In summary, our case describes an acute Influenza B infection that was complicated by pericardial effusion and cardiac tamponade. It also highlights the importance of bedside POCUS and echocardiography in the early diagnosis and treatment of cardiac tamponade cases, frequently with pericardiocentesis as in our case.
甲型和乙型流感急性感染通常主要影响呼吸系统。然而,在罕见情况下,心血管系统也会因病毒的直接作用或既往心脏疾病的恶化而受到损害。我们报告一例罕见的以心包积液和心脏压塞为表现的急性乙型流感感染病例。一名32岁健康女性因流感样症状在急诊室就诊4天,在那里她接受了数小时监测,随后经聚合酶链反应(PCR)检测乙型流感呈阳性后出院回家。第5天,她因症状加重返回急诊室,主要是劳力性呼吸困难。她血压低、心动过速,补液后暂时好转。她被转入重症监护病房,床边即时超声心动图(POCUS)检查以及后来正式的经胸超声心动图检查显示她有心包积液并有心脏压塞的超声征象。紧急进行了心包穿刺术,血流动力学和症状均有改善。最初留置的心包引流管持续引流心包积液(总量700毫升),在超声心动图确认心包积液消退后3天拔除。她完成了为期5天的奥司他韦疗程,随后安全出院回家。总之,我们的病例描述了一例并发心包积液和心脏压塞的急性乙型流感感染。它还强调了床边POCUS和超声心动图在心脏压塞病例早期诊断和治疗中的重要性,如我们的病例中经常需要进行心包穿刺术。