Coomans Marijke B, Dirven Linda, Aaronson Neil K, Baumert Brigitta G, van den Bent Martin, Bottomley Andrew, Brandes Alba A, Chinot Olivier, Coens Corneel, Gorlia Thierry, Herrlinger Ulrich, Keime-Guibert Florence, Malmström Annika, Martinelli Francesca, Sloan Jeff A, Stupp Roger, Talacchi Andrea, Weller Michael, Wick Wolfgang, Reijneveld Jaap C, Taphoorn Martin J B
Department of Neurology, Leiden University Medical Center, Leiden, the Netherlands.
Department of Neurology, Haaglanden Medical Center, Den Haag, the Netherlands.
Neurooncol Adv. 2020 Oct 29;2(1):vdaa147. doi: 10.1093/noajnl/vdaa147. eCollection 2020 Jan-Dec.
Two methods combining survival and health-related quality of life (HRQoL) data in glioma trials to calculate the "net clinical benefit" were evaluated: Quality-adjusted effect sizes (QASES) and joint modeling (JM).
The net clinical benefit in two trials was calculated as proof of concept for other trials. With the QASES method, effect sizes for differences in progression-free survival (PFS) or overall survival (OS) and HRQoL between the experimental arm and standard treatment arm were calculated, while the relative emphasis placed on survival/HRQoL varied. JM allows simultaneous modeling of HRQoL and OS/PFS.
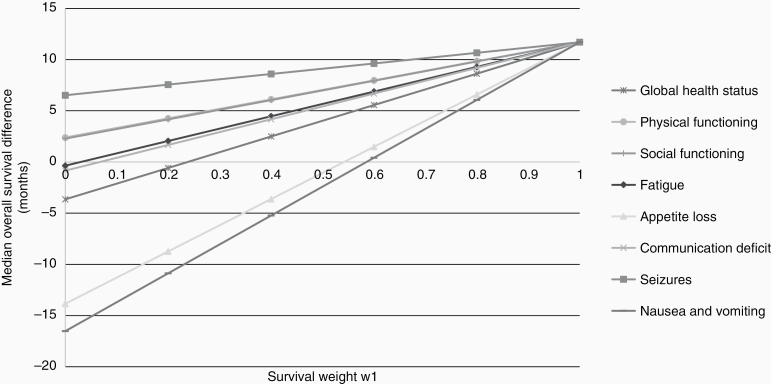
In the EORTC 26951 trial, combined radiochemotherapy significantly prolonged OS (difference 11.7 months), but also resulted in more patients experiencing clinically relevant worsening (≥10 points) in appetite loss and nausea/vomiting shortly after treatment. Using QASES, the survival benefit of additional procarbazine, lomustine, and vincristine (PCV) decreased from 42.3 months to 29.5 and 28.2 months when accounting for appetite loss and nausea/vomiting, respectively. JM analyses resulted in a loss of the beneficial effect of additional PCV between 13% and 24% when adjusting for different HRQoL parameters. The EORTC 22033 trial showed no significant PFS difference between radiotherapy or temozolomide alone (46 vs 39 months), nor clinically relevant differences in HRQoL. JM analyses also showed no significant association between PFS and HRQoL scales/items, whereas QASES showed that temozolomide alone was more favorable when considering symptom burden (47-49 instead of 39 months).
Both methods resulted in different outcomes, but adjusting for the impact of treatment on HRQoL resulted in theoretically reduced survival benefits.
评估了两种在胶质瘤试验中结合生存数据和健康相关生活质量(HRQoL)数据以计算“净临床获益”的方法:质量调整效应量(QASES)和联合建模(JM)。
计算两项试验中的净临床获益作为其他试验的概念验证。使用QASES方法,计算试验组与标准治疗组之间无进展生存期(PFS)或总生存期(OS)差异以及HRQoL的效应量,同时对生存/HRQoL的相对重视程度有所不同。JM允许对HRQoL和OS/PFS进行同时建模。
在欧洲癌症研究与治疗组织(EORTC)26951试验中,联合放化疗显著延长了OS(差异为11.7个月),但也导致更多患者在治疗后不久出现食欲减退和恶心/呕吐方面具有临床意义的恶化(≥10分)。使用QASES,当考虑食欲减退和恶心/呕吐时,额外的丙卡巴肼、洛莫司汀和长春新碱(PCV)的生存获益分别从42.3个月降至29.5个月和28.2个月。当调整不同的HRQoL参数时,JM分析导致额外PCV的有益效果损失13%至24%。EORTC 22033试验显示,单纯放疗或替莫唑胺之间的PFS无显著差异(46对39个月),HRQoL也无临床相关差异。JM分析还显示PFS与HRQoL量表/项目之间无显著关联,而QASES显示,在考虑症状负担时,单纯替莫唑胺更有利(47 - 49个月而非39个月)。
两种方法得出了不同的结果,但调整治疗对HRQoL的影响在理论上导致生存获益降低。