Department of Radiation Oncology, Faculty of Medicine, Martin Luther University Halle-Wittenberg, Ernst-Grube-Straße 40, 06110, Halle (Saale), Germany.
Department of Radiation Oncology, University Medical Center Jena, Jena, Germany.
Strahlenther Onkol. 2021 May;197(5):385-395. doi: 10.1007/s00066-020-01727-4. Epub 2021 Jan 7.
In radical radiochemotherapy (RCT) of inoperable non-small-cell lung cancer (NSCLC) typical prognostic factors include T- and N-stage, while there are still conflicting data on the prognostic relevance of gross tumor volume (GTV) and particularly its changes during RCT. The NCT03055715 study of the Young DEGRO working group of the German Society of Radiation Oncology (DEGRO) evaluated the prognostic impact of GTV and its changes during RCT.
A total of 21 university centers for radiation oncology from five different European countries (Germany, Switzerland, Spain, Belgium, and Austria) participated in the study which evaluated n = 347 patients with confirmed (biopsy) inoperable NSCLC in UICC stage III A/B who received radical curative-intent RCT between 2010 and 2013. Patient and disease data were collected anonymously via electronic case report forms and entered into the multi-institutional RadPlanBio platform for central data analysis. GTV before RCT (initial planning CT, GTV1) and at 40-50 Gy (re-planning CT for radiation boost, GTV2) was delineated. Absolute GTV before/during RCT and relative GTV changes were correlated with overall survival as the primary endpoint. Hazard ratios (HR) of survival analysis were estimated by means of adjusted Cox regression models.
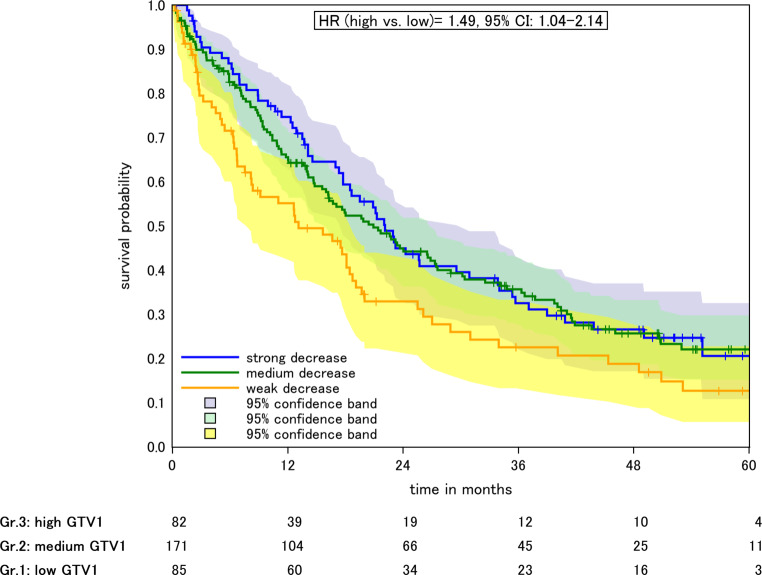
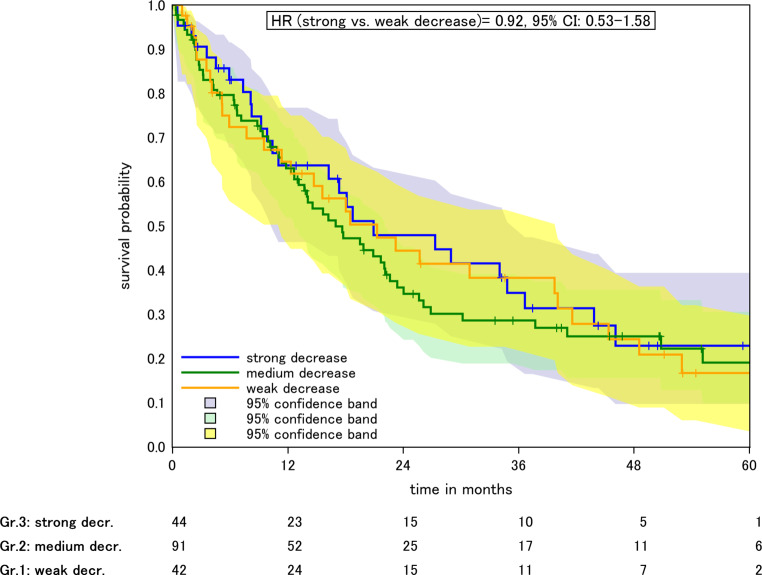
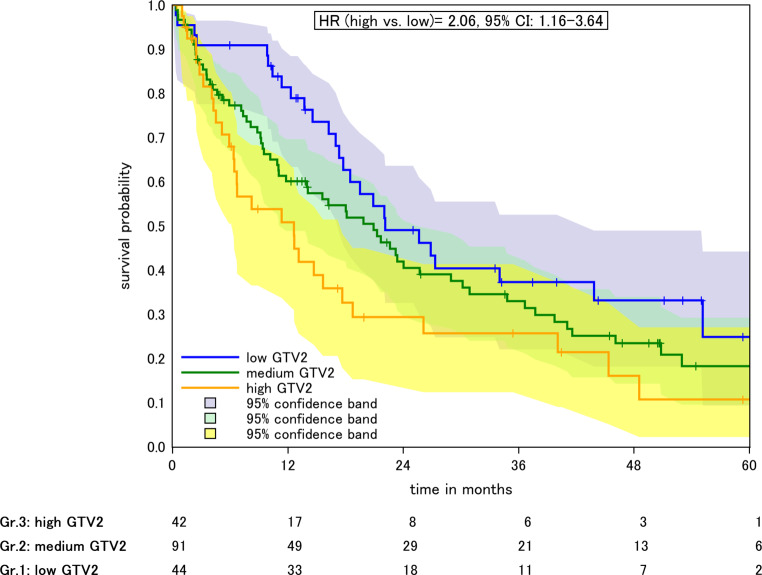
GTV1 was found to have a mean of 154.4 ml (95%CI: 1.5-877) and GTV2 of 106.2 ml (95% CI: 0.5-589.5), resulting in an estimated reduction of 48.2 ml (p < 0.001). Median overall survival (OS) was 18.8 months with a median of 22.1, 20.9, and 12.6 months for patients with high, intermediate, and low GTV before RT. Considering all patients, in one survival model of overall mortality, GTV2 (2.75 (1.12-6.75, p = 0.03) was found to be a stronger survival predictor than GTV1 (1.34 (0.9-2, p > 0.05). In patients with available data on both GTV1 and GTV2, absolute GTV1 before RT was not significantly associated with survival (HR 0-69, 0.32-1.49, p > 0.05) but GTV2 significantly predicted OS in a model adjusted for age, T stage, and chemotherapy, with an HR of 3.7 (1.01-13.53, p = 0.04) per 300 ml. The absolute decrease from GTV1 to GTV2 was correlated to survival, where every decrease by 50 ml reduced the HR by 0.8 (CI 0.64-0.99, p = 0.04). There was no evidence for a survival effect of the relative change between GTV1 and GTV2.
Our results indicate that independently of T stage, the re-planning GTV during RCT is a significant and superior survival predictor compared to baseline GTV before RT. Patients with a high absolute (rather than relative) change in GTV during RT show a superior survival outcome after RCT.
在无法手术的非小细胞肺癌(NSCLC)的根治性放化疗(RCT)中,典型的预后因素包括 T 期和 N 期,而肿瘤体积(GTV)及其在 RCT 期间的变化对预后的相关性仍存在争议。德国放射肿瘤学会(DEGRO)的 Young DEGRO 工作组的 NCT03055715 研究评估了 GTV 及其在 RCT 期间变化的预后影响。
来自五个不同欧洲国家(德国、瑞士、西班牙、比利时和奥地利)的 21 个大学放射肿瘤中心参与了这项研究,共评估了 347 例经组织学证实的(活检)不可手术的 IIIA/B 期非小细胞肺癌患者,这些患者在 2010 年至 2013 年期间接受了根治性 RCT。通过电子病例报告表匿名收集患者和疾病数据,并输入多机构的 RadPlanBio 平台进行中心数据分析。在 RCT 前(初始计划 CT,GTV1)和 40-50Gy 时(放射增敏 CT,GTV2)勾画 GTV。与总生存期(OS)作为主要终点,对 RCT 前后的绝对 GTV 和相对 GTV 变化进行相关性分析。使用调整后的 Cox 回归模型估计生存分析的风险比(HR)。
GTV1 的平均体积为 154.4ml(95%CI:1.5-877),GTV2 的平均体积为 106.2ml(95%CI:0.5-589.5),估计减少了 48.2ml(p<0.001)。中位总生存期(OS)为 18.8 个月,高、中、低 GTV 患者的中位 OS 分别为 22.1、20.9 和 12.6 个月。考虑所有患者,在整体死亡率的一个生存模型中,GTV2(2.75(1.12-6.75,p=0.03)是比 GTV1(1.34(0.9-2,p>0.05)更强的生存预测因子。在有 GTV1 和 GTV2 数据的患者中,RCT 前的绝对 GTV1 与生存无显著相关性(HR 0-69,0.32-1.49,p>0.05),但 GTV2 在调整年龄、T 期和化疗的模型中显著预测 OS,HR 为 3.7(1.01-13.53,p=0.04)每增加 300ml。从 GTV1 到 GTV2 的绝对减少与生存相关,每减少 50ml,HR 降低 0.8(CI 0.64-0.99,p=0.04)。GTV1 和 GTV2 之间的相对变化没有证据表明有生存效果。
我们的结果表明,独立于 T 期,RCT 期间的重新计划 GTV 是比 RCT 前基线 GTV 更显著和优越的生存预测因子。RCT 期间 GTV 绝对值(而非相对值)变化较大的患者,在 RCT 后有更好的生存结果。