Jefferson Headache Center, Thomas Jefferson University, Philadelphia, PA, USA.
Teva Branded Pharmaceutical Products R&D, Inc., West Chester, PA, USA.
J Headache Pain. 2021 Jan 7;22(1):2. doi: 10.1186/s10194-020-01212-4.
Monoclonal antibodies targeting the calcitonin gene-related peptide (CGRP) pathway, including the fully humanized monoclonal antibody (IgG2Δa) fremanezumab, have demonstrated safety and efficacy for migraine prevention. Clinical trials include responders and nonresponders; efficacy outcomes describe mean values across both groups and thus provide little insight into the clinical benefit in responders. Clinicians and their patients want to understand the extent of clinical improvement in patients who respond. This post hoc analysis of fremanezumab treatment attempts to answer this question: what is the benefit in subjects who responded to treatment during the two, phase 3 HALO clinical trials?
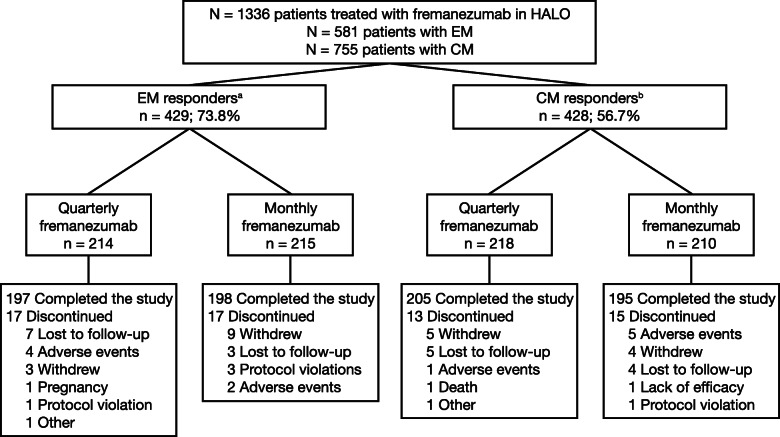
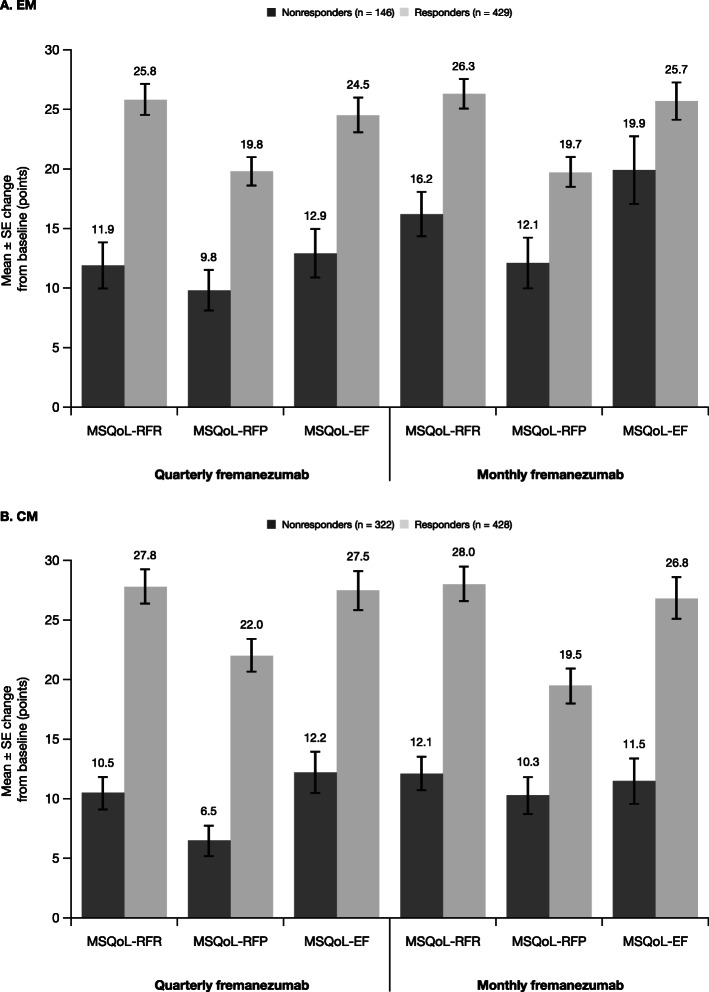
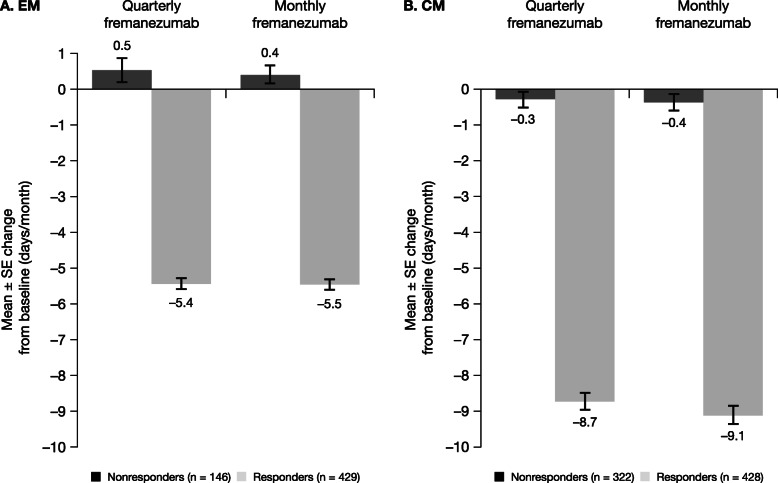
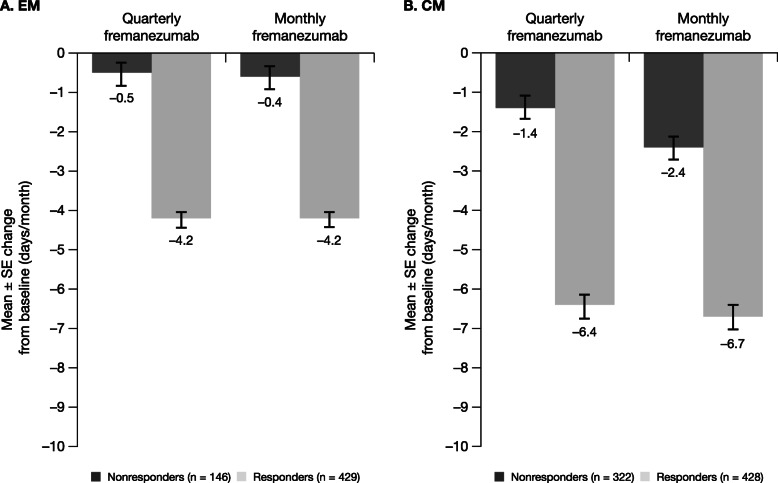
We included subjects with episodic migraine (EM) or chronic migraine (CM) who received fremanezumab quarterly (675 mg/placebo/placebo) or monthly (EM: 225 mg/225 mg/225 mg; CM: 675 mg/225 mg/225 mg) during the 12-week randomized, double-blind, placebo-controlled HALO EM and HALO CM clinical trials. EM and CM responders were defined as participants with a reduction of ≥ 2 or ≥ 4 monthly migraine days, respectively. Treatment benefits evaluated included reductions in monthly migraine days, acute headache medication use, and headache-related disability, and changes in health-related quality of life (HRQoL).
Overall, 857 participants from the HALO trials were identified as responders (EM: 429 [73.8%]; CM: 428 [56.7%]). Reductions in the monthly average number of migraine days were greater among EM (quarterly: 5.4 days; monthly: 5.5 days) and CM (quarterly: 8.7 days; monthly: 9.1 days) responders compared with the overall population. The proportion of participants achieving ≥ 50% reduction in the average monthly number of migraine days was also greater in responders (EM: quarterly, 59.8%; monthly, 63.7%; CM: quarterly, 52.8%; monthly, 59.0%) than in the overall population. Greater reductions in the average number of days of acute headache medication use, greater reductions in headache-related disability scores, and larger improvements in HRQoL were observed among EM and CM responders compared with the overall populations.
Fremanezumab responders achieved clinically meaningful improvements in all outcomes. The magnitude of improvements with fremanezumab across efficacy outcomes was far greater in responders than in the overall trial population, providing insight into expected treatment benefits in participants who respond to fremanezumab in clinical practice.
ClinicalTrials.gov identifiers: NCT02629861 (HALO EM) and NCT02621931 (HALO CM).
靶向降钙素基因相关肽(CGRP)通路的单克隆抗体,包括完全人源化的单克隆抗体(IgG2Δa)fremanezumab,已被证明对偏头痛预防具有安全性和有效性。临床试验包括有反应者和无反应者;疗效结果描述了两组的平均值,因此对有反应者的临床获益几乎没有提供任何见解。临床医生及其患者希望了解对有反应者的患者的临床改善程度。这项 fremanezumab 治疗的事后分析试图回答这个问题:在两项、3 期 HALO 临床试验中,对治疗有反应的受试者中,有什么获益?
我们纳入了接受 fremanezumab 每季度(675mg/安慰剂/安慰剂)或每月(EM:225mg/225mg/225mg;CM:675mg/225mg/225mg)治疗的发作性偏头痛(EM)或慢性偏头痛(CM)患者。EM 和 CM 有反应者的定义为每月偏头痛天数分别减少≥2 或≥4 天的参与者。评估的治疗益处包括每月偏头痛天数、急性头痛药物使用和头痛相关残疾的减少,以及健康相关生活质量(HRQoL)的变化。
总体而言,从 HALO 试验中确定了 857 名有反应者(EM:429 [73.8%];CM:428 [56.7%])。与总体人群相比,EM(每季度:5.4 天;每月:5.5 天)和 CM(每季度:8.7 天;每月:9.1 天)有反应者的每月平均偏头痛天数减少更多。在有反应者中,达到每月平均偏头痛天数减少≥50%的参与者比例也更高(EM:每季度,59.8%;每月,63.7%;CM:每季度,52.8%;每月,59.0%)。与总体人群相比,EM 和 CM 有反应者的急性头痛药物使用天数平均减少更多,头痛相关残疾评分降低更多,HRQoL 改善更大。
fremanezumab 有反应者在所有结局上都取得了有临床意义的改善。在有反应者中,fremanezumab 在疗效结局方面的改善幅度远远大于总体试验人群,为临床实践中对 fremanezumab 有反应的参与者的预期治疗获益提供了深入了解。
ClinicalTrials.gov 标识符:NCT02629861(HALO EM)和 NCT02621931(HALO CM)。