Department of Internal Medicine I, University Hospital Aachen, RWTH Aachen University, Pauwelsstraße 30, 52074, Aachen, Germany.
Center for Translational & Clinical Research Aachen (CTC-A), RWTH Aachen University, Aachen, Germany.
Cardiovasc Diabetol. 2021 Jan 7;20(1):6. doi: 10.1186/s12933-020-01175-5.
In the EMPA-REG OUTCOME trial (Empagliflozin Cardiovascular Outcome Event Trial) treatment with the sodium-glucose cotransporter-2 (SGLT2) inhibitor empagliflozin significantly reduced heart failure hospitalization (HHF) in patients with type 2 diabetes mellitus (T2D) and established cardiovascular disease. The early separation of the HHF event curves within the first 3 months of the trial suggest that immediate hemodynamic effects may play a role. However, hitherto no data exist on early effects of SGLT2 inhibitors on hemodynamic parameters and cardiac function. Thus, this study examined early and delayed effects of empagliflozin treatment on hemodynamic parameters including systemic vascular resistance index, cardiac index, and stroke volume index, as well as echocardiographic measures of cardiac function.
In this placebo-controlled, randomized, double blind, exploratory study patients with T2D were randomized to empagliflozin 10 mg or placebo for a period of 3 months. Hemodynamic and echocardiographic parameters were assessed after 1 day, 3 days and 3 months of treatment.
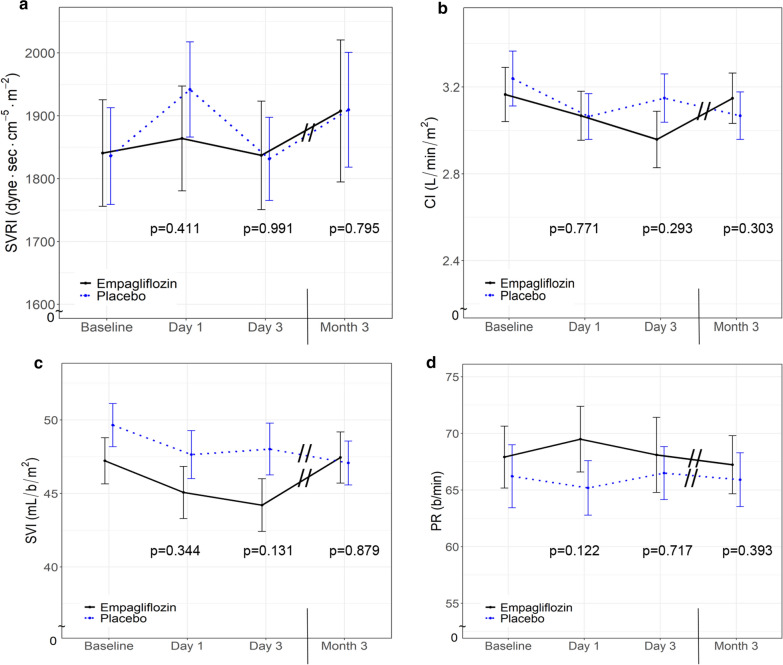
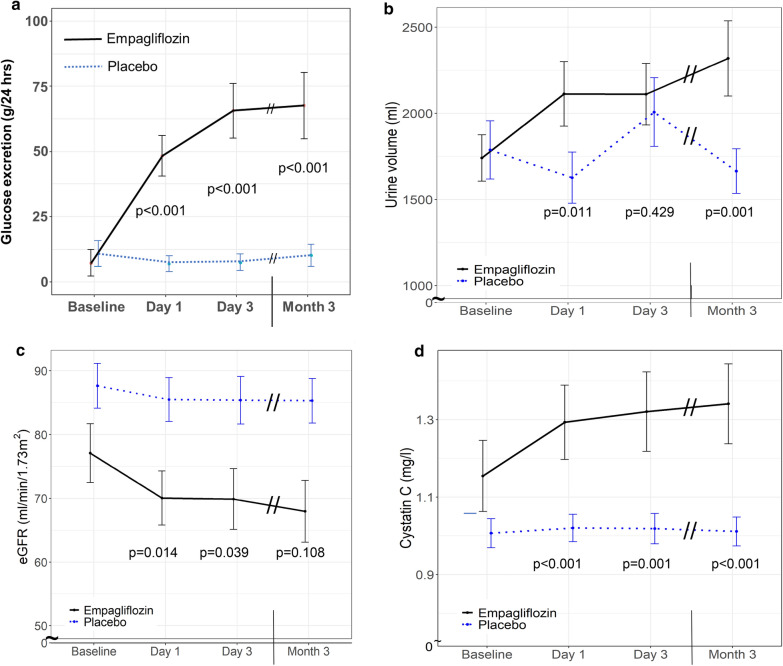
Baseline characteristics were not different in the empagliflozin (n = 22) and placebo (n = 20) group. Empagliflozin led to a significant increase in urinary glucose excretion (baseline: 7.3 ± 22.7 g/24 h; day 1: 48.4 ± 34.7 g/24 h; p < 0.001) as well as urinary volume (1740 ± 601 mL/24 h to 2112 ± 837 mL/24 h; p = 0.011) already after one day compared to placebo. Treatment with empagliflozin had no effect on the primary endpoint of systemic vascular resistance index, nor on cardiac index, stroke volume index or pulse rate at any time point. In addition, echocardiography showed no difference in left ventricular systolic function as assessed by left ventricular ejections fraction and strain analysis. However, empagliflozin significantly improved left ventricular filling pressure as assessed by a reduction of early mitral inflow velocity relative to early diastolic left ventricular relaxation (E/e') which became significant at day 1 of treatment (baseline: 9.2 ± 2.6; day 1: 8.5 ± 2.2; p = 0.005) and remained apparent throughout the study. This was primarily attributable to reduced early mitral inflow velocity E (baseline: 0.8 ± 0.2 m/s; day 1: 0.73 ± 0.2 m/sec; p = 0.003).
Empagliflozin treatment of patients with T2D has no significant effect on hemodynamic parameters after 1 or 3 days, nor after 3 months, but leads to rapid and sustained significant improvement of diastolic function. Trial registration EudraCT Number: 2016-000172-19; date of registration: 2017-02-20 (clinicaltrialregister.eu).
在 EMPA-REG OUTCOME 试验(恩格列净心血管结局事件试验)中,钠-葡萄糖共转运蛋白 2(SGLT2)抑制剂恩格列净显著降低了 2 型糖尿病(T2D)和已确诊心血管疾病患者的心力衰竭住院(HHF)事件。试验开始后前 3 个月内 HHF 事件曲线的早期分离表明,可能存在直接的血液动力学效应。然而,迄今尚无 SGLT2 抑制剂对血液动力学参数和心功能的早期作用的数据。因此,本研究旨在检测恩格列净治疗对血液动力学参数(包括全身血管阻力指数、心指数和每搏输出量指数)以及心脏功能的超声心动图指标的早期和延迟作用。
在这项安慰剂对照、随机、双盲、探索性研究中,将 T2D 患者随机分为恩格列净 10mg 或安慰剂组,治疗时间为 3 个月。在治疗后第 1 天、第 3 天和第 3 个月评估血液动力学和超声心动图参数。
恩格列净组(n=22)和安慰剂组(n=20)的基线特征无差异。与安慰剂相比,恩格列净治疗后尿糖排泄量(基线:7.3±22.7g/24h;第 1 天:48.4±34.7g/24h;p<0.001)和尿量(1740±601mL/24h 至 2112±837mL/24h;p=0.011)均显著增加,且这种增加在第 1 天就已经出现。恩格列净治疗对全身血管阻力指数的主要终点,以及心指数、每搏输出量指数或脉搏率均无影响。此外,超声心动图显示左心室射血分数和应变分析评估的左心室收缩功能无差异。然而,恩格列净可显著降低二尖瓣早期流入速度与舒张早期左心室松弛的比值(E/e'),从而降低左心室充盈压,在治疗第 1 天(基线:9.2±2.6;第 1 天:8.5±2.2;p=0.005)时这一效果具有统计学意义,并且在整个研究过程中均保持明显。这主要归因于二尖瓣早期流入速度 E 的降低(基线:0.8±0.2m/s;第 1 天:0.73±0.2m/sec;p=0.003)。
恩格列净治疗 T2D 患者 1 或 3 天后,以及 3 个月后,对血液动力学参数均无显著影响,但可迅速且持续显著改善舒张功能。
EudraCT 编号:2016-000172-19;注册日期:2017 年 2 月 20 日(clinicaltrialregister.eu)。