Division of Anesthesiology; Department of Anesthesiology, Intensive Care and Pain Medicine, University of Helsinki and Helsinki University Hospital, HUS, P.O. Box 340, FI-00029, Helsinki, Finland.
Department of Emergency Medicine and Services, University of Helsinki and Helsinki University Hospital, HUS, P.O.Box 340, FI-00029, Helsinki, Finland.
Scand J Trauma Resusc Emerg Med. 2021 Jan 7;29(1):13. doi: 10.1186/s13049-020-00816-8.
The challenges encountered in emergency medical services (EMS) contacts with children are likely most pronounced in infants, but little is known about their out-of-hospital care. Our primary aim was to describe the characteristics of EMS contacts with infants. The secondary aims were to examine the symptom-based dispatch system for nonverbal infants, and to observe the association of unfavorable patient outcomes with patient and EMS mission characteristics.
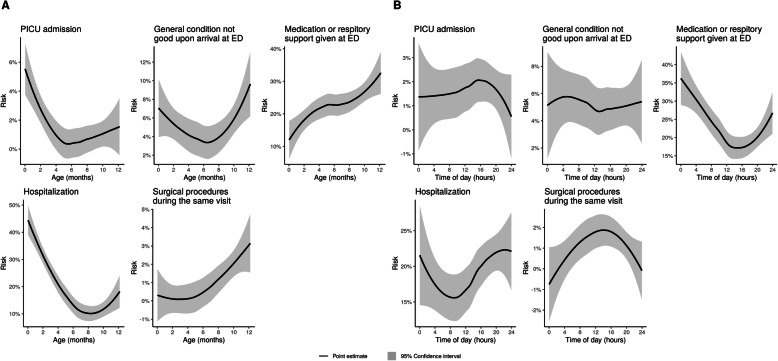
In a population-based 5-year retrospective cohort of all 1712 EMS responses for infants (age < 1 year) in Helsinki, Finland (population 643,000, < 1-year old population 6548), we studied 1) the characteristics of EMS missions with infants; 2) mortality within 12 months; 3) pediatric intensive care unit (PICU) admissions; 4) medical state of the infant upon presentation to the emergency department (ED); 5) any medication or respiratory support given at the ED; 6) hospitalization; and 7) surgical procedures during the same hospital visit.
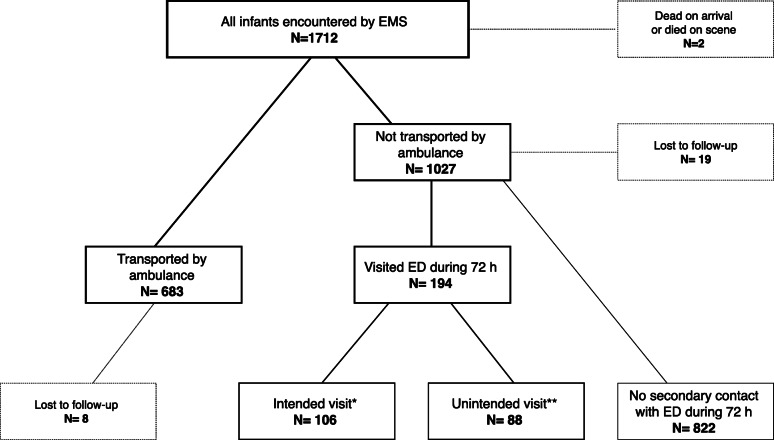
1712 infants with a median age of 6.7 months were encountered, comprising 0.4% of all EMS missions. The most common complaints were dyspnea, low-energy falls, and choking. Two infants died on-scene. The EMS transported 683 (39.9%) infants. One (0.1%) infant died during the 12-month follow-up period. Ninety-one infants had abnormal clinical examination upon arrival at the ED. PICU admissions (n = 28) were associated with young age (P < 0.01), a history of prematurity or problems in the neonatal period (P = 0.01), and previous EMS contacts within 72 h (P = 0.04). The adult-derived dispatch codes did not associate with the final diagnoses of the infants.
Infants form a small but distinct group in pediatric EMS care, with specific characteristics differing from the overall pediatric population. Many EMS contacts with infants were nonurgent or medically unjustified, possibly reflecting an unmet need for other family services. The use of adult-derived symptom codes for dispatching is not optimal for infants. Unfavorable patient outcomes were rare. Risk factors for such outcomes include quickly renewed contacts, young age and health problems in the neonatal period.
在紧急医疗服务(EMS)接触儿童时遇到的挑战在婴儿中可能最为明显,但对于他们的院外护理知之甚少。我们的主要目的是描述与婴儿接触的 EMS 的特征。次要目的是检查非言语婴儿的基于症状的调度系统,并观察不良患者结局与患者和 EMS 任务特征的关联。
在芬兰赫尔辛基的一项基于人群的 5 年回顾性队列研究中,我们研究了所有 1712 名年龄在 1 岁以下(年龄 < 1 岁)的婴儿的 EMS 反应(人口 643000,< 1 岁的人口 6548):1)与婴儿接触的 EMS 任务特征;2)12 个月内的死亡率;3)儿科重症监护病房(PICU)入院;4)到达急诊部(ED)时婴儿的医疗状况;5)在 ED 给予的任何药物或呼吸支持;6)住院;以及 7)同一医院就诊期间的手术。
共遇到 1712 名婴儿,中位年龄为 6.7 个月,占所有 EMS 任务的 0.4%。最常见的投诉是呼吸困难、低能量跌倒和窒息。两名婴儿在现场死亡。EMS 运送了 683 名(39.9%)婴儿。一名(0.1%)婴儿在 12 个月的随访期间死亡。91 名婴儿在到达 ED 时临床检查异常。PICU 入院(n=28)与年龄较小(P < 0.01)、早产或新生儿期问题史(P=0.01)和 72 小时内之前的 EMS 接触(P=0.04)相关。成人衍生的调度代码与婴儿的最终诊断无关。
婴儿在儿科 EMS 护理中形成一个较小但独特的群体,具有与整体儿科人群不同的特定特征。许多与婴儿的 EMS 接触是非紧急或没有医学依据的,这可能反映了对其他家庭服务的未满足需求。使用成人衍生的症状代码进行调度对于婴儿来说并不理想。不良患者结局很少见。这些结局的危险因素包括迅速恢复接触、年龄较小和新生儿期健康问题。