Szturz Petr, Nevens Daan, Vermorken Jan B
Medical Oncology, Department of Oncology, Lausanne University Hospital (CHUV), Lausanne, Switzerland.
Department of Radiation Oncology, IridiumNetwork, Wilrijk (Antwerp), Belgium.
Front Oncol. 2020 Dec 22;10:617793. doi: 10.3389/fonc.2020.617793. eCollection 2020.
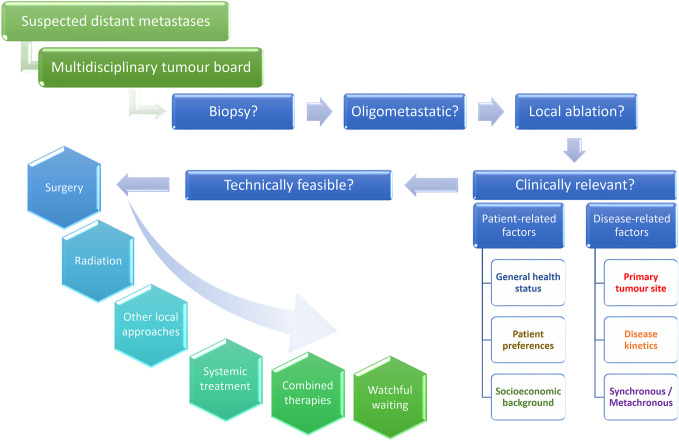
Hematogenous dissemination represents a common manifestation of squamous cell carcinoma of the head and neck, and the recommended therapeutic options usually consist of systemically administered drugs with palliative intent. However, mounting evidence suggests that patients with few and slowly progressive distant lesions of small size may benefit from various local ablation techniques, which have already been established as standard-of-care modalities for example in colorectal and renal cell carcinomas and in sarcomas. In principle, serving as radical approaches to eradicate cancer, these interventions can be curative. Their impact on local control and overall survival has been shown in numerous retrospective and prospective studies. The term oligometastatic refers to the number of distant lesions which should generally not surpass five in total, ideally in one organ. Currently, surgical resection remains the method of choice supported by the majority of published data. More recently, stereotactic (ablative) body radiotherapy (SABR/SBRT) has emerged as a viable alternative. In cases technically amenable to such local interventions, several other clinical variables need to be taken into account also, including patient-related factors (general health status, patient preferences, socioeconomic background) and disease-related factors (primary tumor site, growth kinetics, synchronous or metachronous metastases). In head and neck cancer, patients presenting with late development of slowly progressive oligometastatic lesions in the lungs secondary to human papillomavirus (HPV)-positive oropharyngeal cancer are the ideal candidates for metastasectomy or other local therapies. However, literature data are still limited to say whether there are other subgroups benefiting from this approach. One of the plausible explanations is that radiological follow-up after primary curative therapy is usually not recommended because its impact on survival has not been unequivocal, which is also due to the rarity of oligometastatic manifestations in this disease. At the same time, aggressive treatment of synchronous metastases early in the disease course should be weighed against the risk of futile interventions in a disease with already multimetastatic microscopic dissemination. Therefore, attentive treatment sequencing, meticulous appraisal of cancer extension, refinement of post-treatment surveillance, and understanding of tumor biology and kinetics are crucial in the management of oligometastases.
血行播散是头颈部鳞状细胞癌的常见表现,推荐的治疗方案通常包括以姑息为目的的全身给药。然而,越来越多的证据表明,远处病灶数量少且进展缓慢、体积小的患者可能从各种局部消融技术中获益,这些技术已成为结直肠癌、肾细胞癌和肉瘤等疾病的标准治疗方式。原则上,作为根除癌症的根治性方法,这些干预措施可以治愈。它们对局部控制和总生存的影响已在众多回顾性和前瞻性研究中得到证实。寡转移一词指的是远处病灶的数量,总数一般不应超过五个,理想情况下是在一个器官内。目前,手术切除仍然是大多数已发表数据支持的首选方法。最近,立体定向(消融)体部放疗(SABR/SBRT)已成为一种可行的替代方法。在技术上适合这种局部干预的病例中,还需要考虑其他几个临床变量,包括患者相关因素(一般健康状况、患者偏好、社会经济背景)和疾病相关因素(原发肿瘤部位、生长动力学、同时性或异时性转移)。在头颈部癌中,继发于人乳头瘤病毒(HPV)阳性口咽癌的肺部缓慢进展的寡转移病灶出现较晚的患者是转移灶切除术或其他局部治疗的理想候选者。然而,关于是否有其他亚组患者能从这种方法中获益,文献数据仍然有限。一个合理的解释是,通常不建议在初次根治性治疗后进行放射学随访,因为其对生存的影响尚不明确,这也是由于该疾病中寡转移表现罕见所致。同时,在疾病进程早期积极治疗同时性转移应权衡在已有多灶微小播散疾病中进行无效干预的风险。因此,在寡转移的管理中,精心安排治疗顺序、细致评估癌症范围、完善治疗后监测以及了解肿瘤生物学和动力学至关重要。