Department of General Pediatrics, Neonatology and Pediatric Cardiology, University Children's Hospital, Medical Faculty, Heinrich-Heine-University Duesseldorf, Duesseldorf, Germany.
Front Endocrinol (Lausanne). 2020 Nov 30;11:580642. doi: 10.3389/fendo.2020.580642. eCollection 2020.
Aim was to identify hypotheses why adverse neurodevelopment still occurs in children with transient or persistent hyperinsulinism despite improvements in long-term treatment options during the last decades.
A retrospective review of 87 children with transient (n=37) or persistent congenital hyperinsulinism (CHI) (n=50) was conducted at the University Children's Hospital Duesseldorf, Germany. Possible risk factors for neurodevelopmental sequelae due to hypoglycemia were analyzed with a focus on the first days after onset of disease.
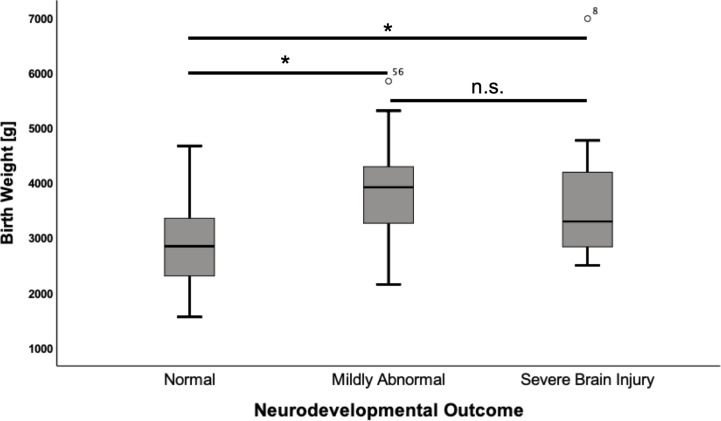
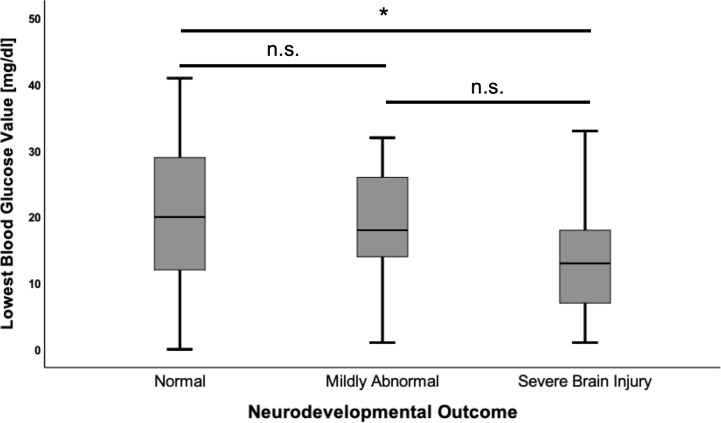
Median age at follow-up was 7 years (IQR 8). Adverse neurodevelopmental outcome was seen in 34.5% (n=30) of all CHI patients. Fifteen had mildly abnormal neurodevelopment and 15 had a severe hypoglycemic brain injury. In univariate analysis, mildly abnormal neurodevelopment was associated with the diagnosis of persistent CHI (odds ratio (OR) 8.3; p=0.004) and higher birth weight (mean difference 1049 g; p<0.001). Severe hypoglycemic brain injury was associated with the diagnosis of persistent CHI (OR 5.1; p=0.013), being born abroad (OR 18.3; p<0.001) or in a lower-level maternity hospital (OR 4.8; p=0.039), and of note history of hypoglycemic seizures (OR 13.0; p=<0.001), and a delay between first symptoms of hypoglycemia and first blood glucose measurement/initiation of treatment (OR 10.7; p<0.001). Children with severe hypoglycemic brain injury had lower recorded blood glucose (mean difference -8.34 mg/dl; p=0.022) and higher birth weight than children with normal development (mean difference 829 g; p=0.012). In multivariate binary logistic regression models, lowest blood glucose <20 mg/dl (OR 134.3; p=0.004), a delay between initial symptoms and first blood glucose measurement/initiation of treatment (OR 71.7; p=0.017) and hypoglycemic seizures (OR 12.9; p=0.008) were positively correlated with severe brain injury. Analysis showed that the odds for brain injury decreased by 15% (OR 0.85; p=0.035) if the blood glucose increased by one unit.
While some risk factors for adverse outcome in CHI are not influenceable, others like lowest recorded blood glucose values <20 mg/dl, hypoglycemic seizures, and insufficiently-or even untreated hypoglycemia can be avoided. Future guidelines for management of neonatal hypoglycemia should address this by ensuring early identification and immediate treatment with appropriate escalation steps.
尽管在过去几十年中,针对永久性和暂时性高胰岛素血症的长期治疗选择有所改进,但仍有部分患儿存在神经发育不良的情况,本研究旨在探寻其中的原因。
本研究回顾性分析了德国杜塞尔多夫儿童大学医院 87 名患有暂时性(n=37)或永久性先天性高胰岛素血症(CHI)(n=50)患儿的临床资料。重点分析了疾病发作后最初几天内导致低血糖的可能危险因素。
随访中位数年龄为 7 岁(IQR 8)。所有 CHI 患儿中,有 34.5%(n=30)出现不良神经发育结局。其中 15 例患儿存在轻度神经发育异常,15 例存在严重低血糖性脑损伤。单因素分析显示,轻度神经发育异常与永久性 CHI (比值比(OR)8.3;p=0.004)和较高的出生体重(平均差异 1049g;p<0.001)相关。严重低血糖性脑损伤与永久性 CHI (OR 5.1;p=0.013)、在国外(OR 18.3;p<0.001)或低级别产科医院(OR 4.8;p=0.039)出生、低血糖性癫痫发作史(OR 13.0;p<0.001)、低血糖发作至首次血糖测量/治疗开始之间的时间延迟(OR 10.7;p<0.001)有关。严重低血糖性脑损伤患儿的记录血糖值较低(平均差异 -8.34mg/dl;p=0.022),出生体重较高(平均差异 829g;p=0.012)。多变量二项逻辑回归模型分析显示,血糖值最低 <20mg/dl(OR 134.3;p=0.004)、低血糖发作(OR 12.9;p=0.008)和血糖测量/治疗延迟(OR 71.7;p=0.017)与严重脑损伤呈正相关。分析表明,如果血糖升高 1 单位,脑损伤的几率会降低 15%(OR 0.85;p=0.035)。
尽管某些 CHI 不良预后的危险因素不可改变,但其他因素,如记录的血糖值最低 <20mg/dl、低血糖发作和治疗不充分甚至未治疗的低血糖,是可以避免的。未来的新生儿低血糖管理指南应通过确保早期识别和立即采用适当的升级步骤来治疗,以解决这个问题。