Lak Hassan, Rehman Karim Abdul, Jaber Wael A, Cho Leslie
Department of Medicine, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195, USA.
Robert and Suzanne Tomsich Department of Cardiovascular Medicine, Heart, Vascular and Thoracic Institute, Cleveland Clinic, Mail Code JB-1, 9500 Euclid Avenue, Cleveland, OH 44195, USA.
Eur Heart J Case Rep. 2020 Sep 18;4(5):1-6. doi: 10.1093/ehjcr/ytaa319. eCollection 2020 Oct.
Spontaneous coronary artery dissection (SCAD) is a frequently underdiagnosed entity that carries a significant risk of morbidity and mortality. Spontaneous coronary artery dissection is increasingly recognized as an important cause of acute coronary syndrome (ACS) and, the majority of SCAD patients are young healthy women.
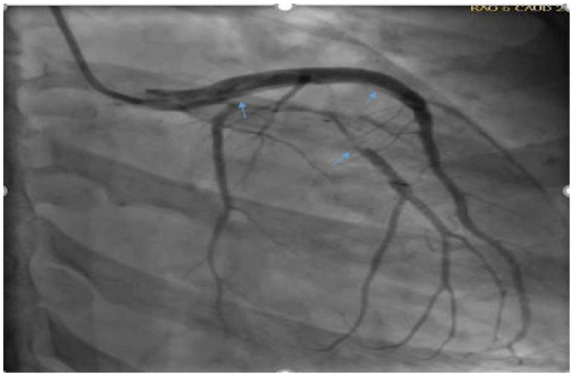
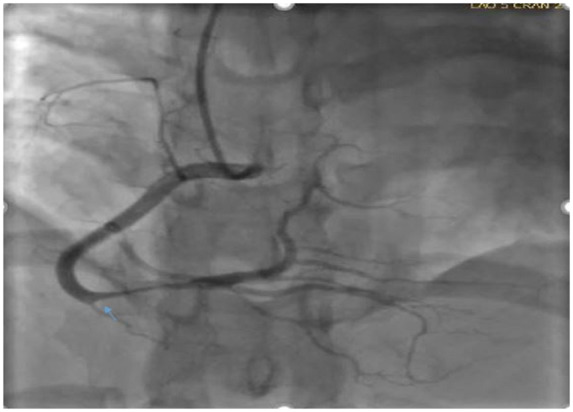
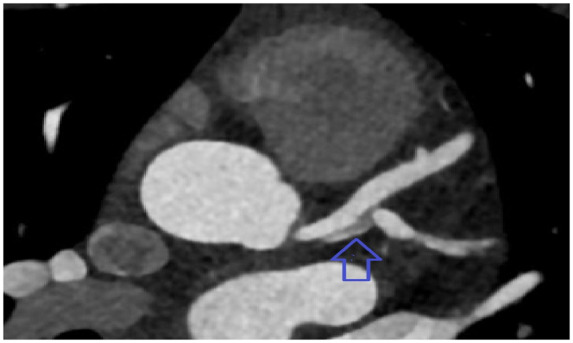
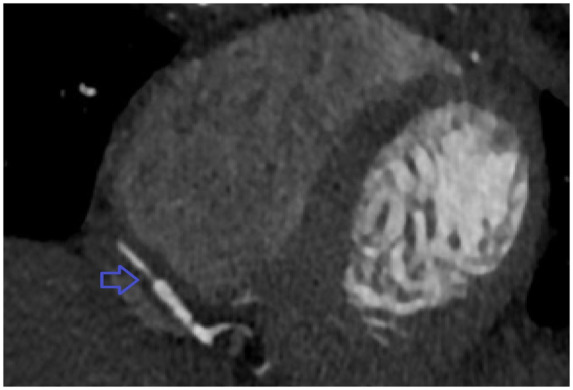
A 23-year-old female G5P4 presented to the emergency room for severe sub-sternal chest pain, associated with shortness of breath. Past medical history was significant for pre-eclampsia. Initial electrocardiogram was remarkable for ST depressions in V5-V6 with inverted T waves to V1-V2. Troponin I was elevated to 1.13 ng/mL. Two-dimensional echo showed reduced left ventricular function with an ejection fraction of 40%. Cardiac catheterization showed triple vessel dissection involving the left main trunk extending into mid-left anterior descending and dissection extending from ostium of left circumflex artery into large first obtuse marginal branch. She was started on aspirin and heparin. After 48 h she was loaded with clopidogrel. Computed tomography angiography of head, neck, abdomen, and pelvis showed findings compatible with fibromuscular dysplasia. She was haemodynamically stable and symptom free and did not want surgery. She was recommended to continue dual antiplatelet therapy for 12 months and subsequently aspirin and beta blocker only lifelong.
Spontaneous coronary artery dissection is a rare condition which is underdiagnosed. A thorough history and high degree of suspicion is required to diagnose in a timely manner and it should be high on differential in a postpartum female presenting with signs and symptoms of ACS.
自发性冠状动脉夹层(SCAD)是一种常被漏诊的疾病,具有较高的发病和死亡风险。自发性冠状动脉夹层日益被认为是急性冠状动脉综合征(ACS)的重要病因,且大多数SCAD患者为年轻健康女性。
一名23岁、孕5产4的女性因严重胸骨后胸痛伴呼吸急促就诊于急诊室。既往病史有子痫前期。初始心电图显示V5-V6导联ST段压低,V1-V2导联T波倒置。肌钙蛋白I升高至1.13 ng/mL。二维超声心动图显示左心室功能降低,射血分数为40%。心脏导管检查显示三支血管夹层,累及左主干并延伸至左前降支中段,夹层从左旋支动脉开口延伸至大的第一钝缘支。给予阿司匹林和肝素治疗。48小时后给予氯吡格雷负荷剂量。头、颈、腹和盆腔的计算机断层血管造影显示结果与纤维肌发育不良相符。她血流动力学稳定且无症状,不希望接受手术。建议她继续双联抗血小板治疗12个月,随后终身服用阿司匹林和β受体阻滞剂。
自发性冠状动脉夹层是一种罕见且易被漏诊的疾病。需要详细的病史和高度的怀疑才能及时诊断,对于出现ACS症状和体征的产后女性,应将其列为鉴别诊断的重点。