Northern Institute for Cancer Research, Newcastle University, Newcastle upon Tyne, United Kingdom.
The Institute of Cancer Research, London, United Kingdom.
PLoS Med. 2021 Jan 11;18(1):e1003454. doi: 10.1371/journal.pmed.1003454. eCollection 2021 Jan.
Carfilzomib is a second-generation irreversible proteasome inhibitor that is efficacious in the treatment of myeloma and carries less risk of peripheral neuropathy than first-generation proteasome inhibitors, making it more amenable to combination therapy.
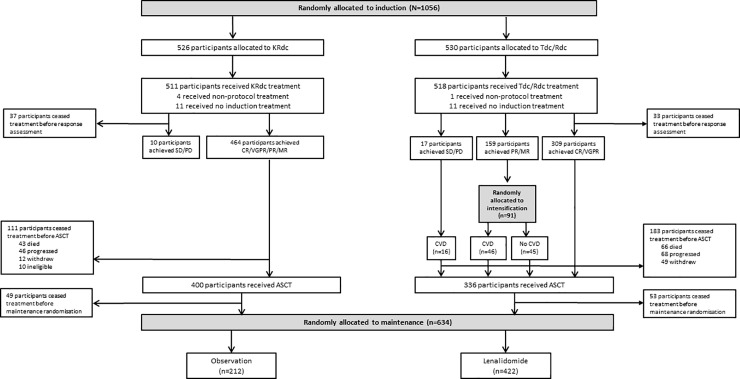
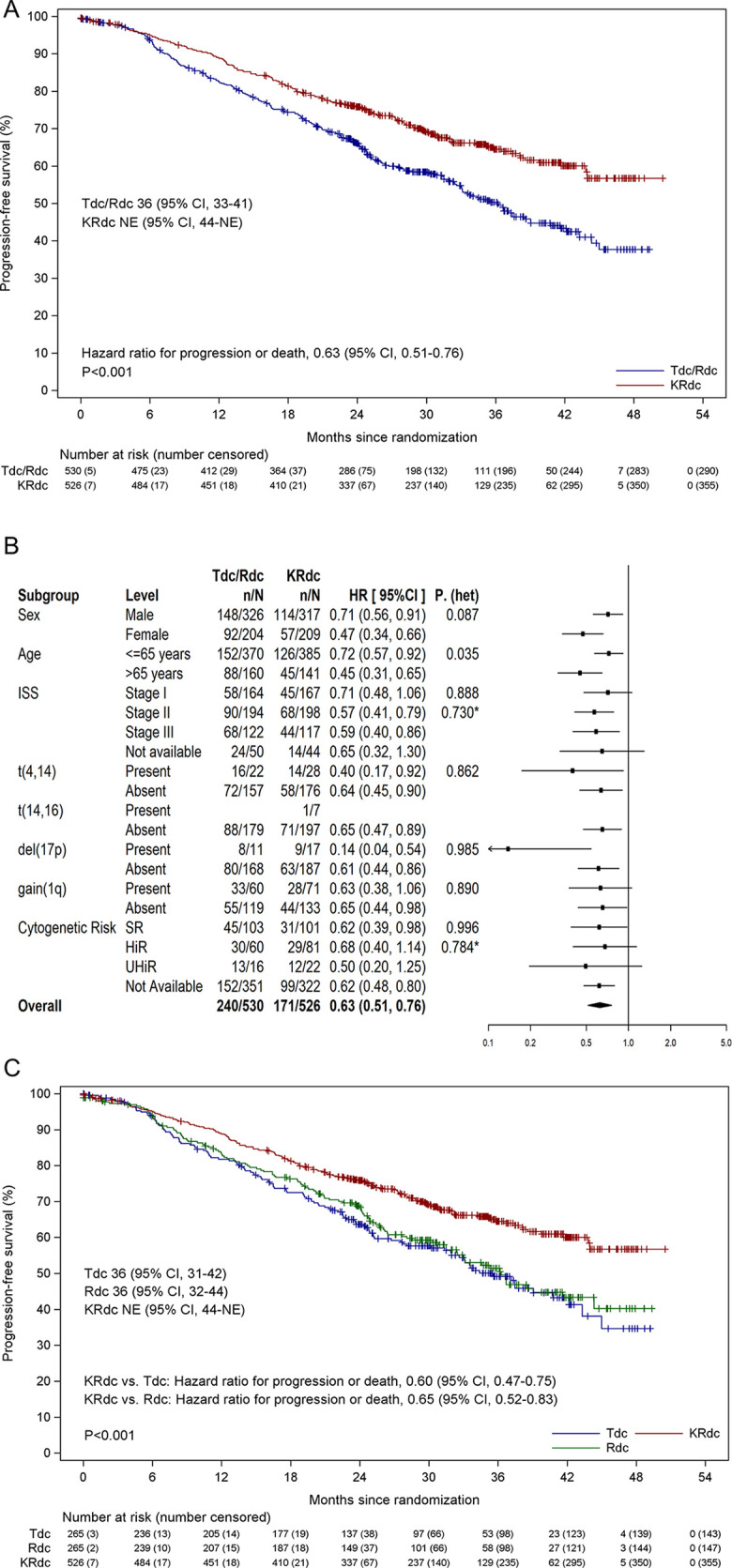
The Myeloma XI+ trial recruited patients from 88 sites across the UK between 5 December 2013 and 20 April 2016. Patients with newly diagnosed multiple myeloma eligible for transplantation were randomly assigned to receive the combination carfilzomib, lenalidomide, dexamethasone, and cyclophosphamide (KRdc) or a triplet of lenalidomide, dexamethasone, and cyclophosphamide (Rdc) or thalidomide, dexamethasone, and cyclophosphamide (Tdc). All patients were planned to receive an autologous stem cell transplantation (ASCT) prior to a randomisation between lenalidomide maintenance and observation. Eligible patients were aged over 18 years and had symptomatic myeloma. The co-primary endpoints for the study were progression-free survival (PFS) and overall survival (OS) for KRdc versus the Tdc/Rdc control group by intention to treat. PFS, response, and safety outcomes are reported following a planned interim analysis. The trial is registered (ISRCTN49407852) and has completed recruitment. In total, 1,056 patients (median age 61 years, range 33 to 75, 39.1% female) underwent induction randomisation to KRdc (n = 526) or control (Tdc/Rdc, n = 530). After a median follow-up of 34.5 months, KRdc was associated with a significantly longer PFS than the triplet control group (hazard ratio 0.63, 95% CI 0.51-0.76). The median PFS for patients receiving KRdc is not yet estimable, versus 36.2 months for the triplet control group (p < 0.001). Improved PFS was consistent across subgroups of patients including those with genetically high-risk disease. At the end of induction, the percentage of patients achieving at least a very good partial response was 82.3% in the KRdc group versus 58.9% in the control group (odds ratio 4.35, 95% CI 3.19-5.94, p < 0.001). Minimal residual disease negativity (cutoff 4 × 10-5 bone marrow leucocytes) was achieved in 55% of patients tested in the KRdc group at the end of induction, increasing to 75% of those tested after ASCT. The most common adverse events were haematological, with a low incidence of cardiac events. The trial continues to follow up patients to the co-primary endpoint of OS and for planned long-term follow-up analysis. Limitations of the study include a lack of blinding to treatment regimen and that the triplet control regimen did not include a proteasome inhibitor for all patients, which would be considered a current standard of care in many parts of the world.
The KRdc combination was well tolerated and was associated with both an increased percentage of patients achieving at least a very good partial response and a significant PFS benefit compared to immunomodulatory-agent-based triplet therapy.
ClinicalTrials.gov ISRCTN49407852.
卡非佐米是一种第二代不可逆蛋白酶体抑制剂,在治疗骨髓瘤方面具有疗效,并且比第一代蛋白酶体抑制剂发生周围神经病的风险更小,因此更适合联合治疗。
多发性骨髓瘤 XI+试验于 2013 年 12 月 5 日至 2016 年 4 月 20 日期间在英国的 88 个地点招募患者。有资格接受移植的新诊断多发性骨髓瘤患者被随机分配接受卡非佐米、来那度胺、地塞米松和环磷酰胺联合治疗(KRdc)或来那度胺、地塞米松和环磷酰胺三联治疗(Rdc)或沙利度胺、地塞米松和环磷酰胺联合治疗(Tdc)。所有患者均计划在随机分组接受来那度胺维持治疗或观察治疗之前接受自体干细胞移植(ASCT)。该研究的主要共同终点是 KRdc 与 Tdc/Rdc 对照组的无进展生存期(PFS)和总生存期(OS),以意向治疗为基础。在计划的中期分析后报告 PFS、反应和安全性结果。该试验已注册(ISRCTN49407852)并已完成招募。共有 1056 名患者(中位年龄 61 岁,范围 33-75 岁,39.1%为女性)接受诱导随机分配至 KRdc(n=526)或对照组(Tdc/Rdc,n=530)。在中位随访 34.5 个月后,KRdc 与对照组(Tdc/Rdc)相比,PFS 显著延长(风险比 0.63,95%CI 0.51-0.76)。接受 KRdc 治疗的患者的中位 PFS 尚未可估计,而对照组的中位 PFS 为 36.2 个月(p<0.001)。在包括遗传高危疾病在内的患者亚组中,均观察到 PFS 改善。在诱导结束时,KRdc 组至少达到非常好的部分缓解的患者比例为 82.3%,而对照组为 58.9%(优势比 4.35,95%CI 3.19-5.94,p<0.001)。在诱导结束时,KRdc 组 55%的患者达到了最小残留疾病阴性(骨髓白细胞 4×10-5),在接受 ASCT 后,这一比例增加到 75%。最常见的不良事件是血液学事件,心脏事件发生率较低。该试验继续对患者进行随访,以达到主要共同终点 OS 和计划进行长期随访分析。该研究的局限性包括治疗方案缺乏盲法,以及对照组的三联方案并非对所有患者都包含蛋白酶体抑制剂,这在世界许多地区被认为是目前的标准治疗方法。
KRdc 联合治疗耐受性良好,与基于免疫调节剂的三联治疗相比,不仅可使更多的患者至少达到非常好的部分缓解,而且还可显著延长 PFS。
ClinicalTrials.gov ISRCTN49407852。