Armengol Marc, Santos Juliana Carvalho, Fernández-Serrano Miranda, Profitós-Pelejà Núria, Ribeiro Marcelo Lima, Roué Gaël
Lymphoma Translational Group, Josep Carreras Leukaemia Research Institute (IJC), 08916 Badalona, Spain.
Laboratory of Immunopharmacology and Molecular Biology, Sao Francisco University Medical School, Braganca Paulista, São Paulo 01246-100, Brazil.
Cancers (Basel). 2021 Jan 8;13(2):214. doi: 10.3390/cancers13020214.
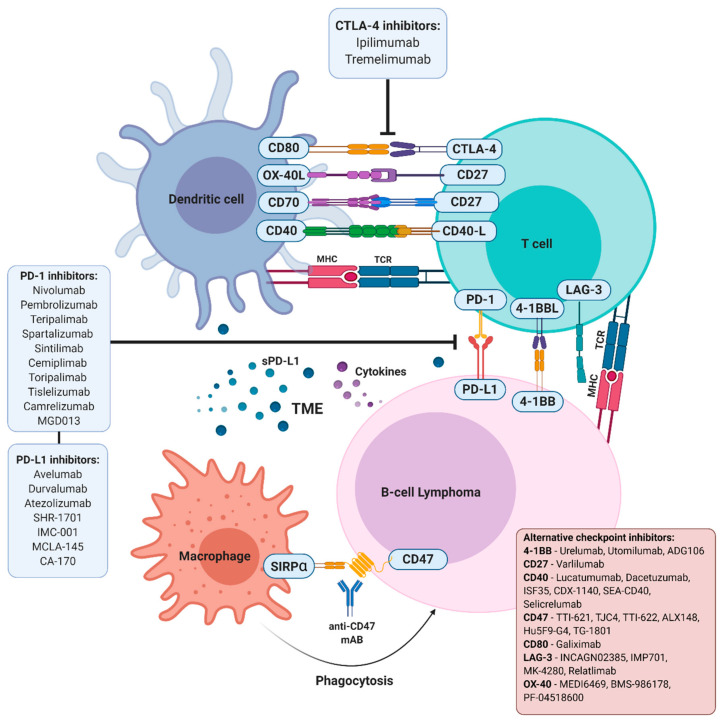
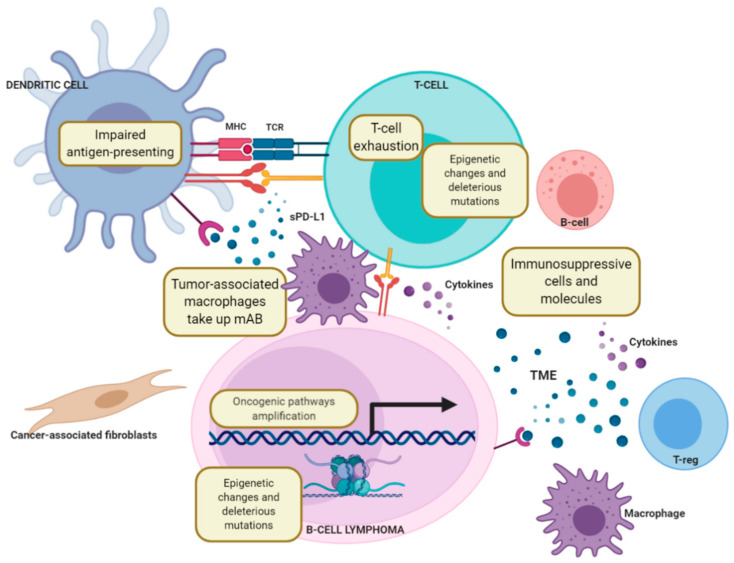
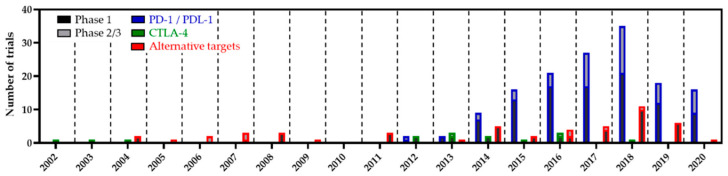
For years, immunotherapy has been considered a viable and attractive treatment option for patients with cancer. Among the immunotherapy arsenal, the targeting of intratumoral immune cells by immune-checkpoint inhibitory agents has recently revolutionised the treatment of several subtypes of tumours. These approaches, aimed at restoring an effective antitumour immunity, rapidly reached the market thanks to the simultaneous identification of inhibitory signals that dampen an effective antitumor response in a large variety of neoplastic cells and the clinical development of monoclonal antibodies targeting checkpoint receptors. Leading therapies in solid tumours are mainly focused on the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed death 1 (PD-1) pathways. These approaches have found a promising testing ground in both Hodgkin lymphoma and non-Hodgkin lymphoma, mainly because, in these diseases, the malignant cells interact with the immune system and commonly provide signals that regulate immune function. Although several trials have already demonstrated evidence of therapeutic activity with some checkpoint inhibitors in lymphoma, many of the immunologic lessons learned from solid tumours may not directly translate to lymphoid malignancies. In this sense, the mechanisms of effective antitumor responses are different between the different lymphoma subtypes, while the reasons for this substantial difference remain partially unknown. This review will discuss the current advances of immune-checkpoint blockade therapies in B-cell lymphoma and build a projection of how the field may evolve in the near future. In particular, we will analyse the current strategies being evaluated both preclinically and clinically, with the aim of fostering the use of immune-checkpoint inhibitors in lymphoma, including combination approaches with chemotherapeutics, biological agents and/or different immunologic therapies.
多年来,免疫疗法一直被认为是癌症患者可行且有吸引力的治疗选择。在免疫疗法的武器库中,免疫检查点抑制剂对肿瘤内免疫细胞的靶向作用最近彻底改变了几种肿瘤亚型的治疗方式。这些旨在恢复有效的抗肿瘤免疫力的方法,由于同时识别出抑制多种肿瘤细胞中有效抗肿瘤反应的抑制信号以及靶向检查点受体的单克隆抗体的临床开发,迅速进入市场。实体瘤的主要治疗方法主要集中在细胞毒性T淋巴细胞相关抗原4(CTLA-4)和程序性死亡1(PD-1)途径。这些方法在霍奇金淋巴瘤和非霍奇金淋巴瘤中都找到了有前景的试验场,主要是因为在这些疾病中,恶性细胞与免疫系统相互作用,通常会提供调节免疫功能的信号。尽管一些试验已经证明了某些检查点抑制剂在淋巴瘤中的治疗活性证据,但从实体瘤中学到的许多免疫学经验可能无法直接转化为淋巴系统恶性肿瘤。从这个意义上说,不同淋巴瘤亚型之间有效抗肿瘤反应的机制不同,而这种巨大差异的原因仍部分未知。本综述将讨论免疫检查点阻断疗法在B细胞淋巴瘤中的当前进展,并对该领域在不久的将来可能如何发展进行预测。特别是,我们将分析目前正在临床前和临床评估的策略,以促进免疫检查点抑制剂在淋巴瘤中的应用,包括与化疗药物、生物制剂和/或不同免疫疗法的联合方法。