Department of Anesthesiology, Erasme Hospital, Université Libre de Bruxelles, Brussels, Belgium.
Department of Anesthesiology and Intensive Care, Hôpitaux Universitaires Paris-Sud, Université Paris-Sud, Université Paris-Saclay, Paul Brousse Hospital, Assistance Publique Hôpitaux de Paris (APHP), 12 Avenue Paul Vaillant Couturier, 94800, Villejuif, France.
BMC Anesthesiol. 2021 Jan 11;21(1):12. doi: 10.1186/s12871-020-01228-y.
Acute kidney injury (AKI) occurs frequently after liver transplant surgery and is associated with significant morbidity and mortality. While the impact of intraoperative hypotension (IOH) on postoperative AKI has been well demonstrated in patients undergoing a wide variety of non-cardiac surgeries, it remains poorly studied in liver transplant surgery. We tested the hypothesis that IOH is associated with AKI following liver transplant surgery.
This historical cohort study included all patients who underwent liver transplant surgery between 2014 and 2019 except those with a preoperative creatinine > 1.5 mg/dl and/or who had combined transplantation surgery. IOH was defined as any mean arterial pressure (MAP) < 65 mmHg and was classified according to the percentage of case time during which the MAP was < 65 mmHg into three groups, based on the interquartile range of the study cohort: "short" (Quartile 1, < 8.6% of case time), "intermediate" (Quartiles 2-3, 8.6-39.5%) and "long" (Quartile 4, > 39.5%) duration. AKI stages were classified according to a "modified" "Kidney Disease: Improving Global Outcomes" (KDIGO) criteria. Logistic regression modelling was conducted to assess the association between IOH and postoperative AKI. The model was run both as a univariate and with multiple perioperative covariates to test for robustness to confounders.
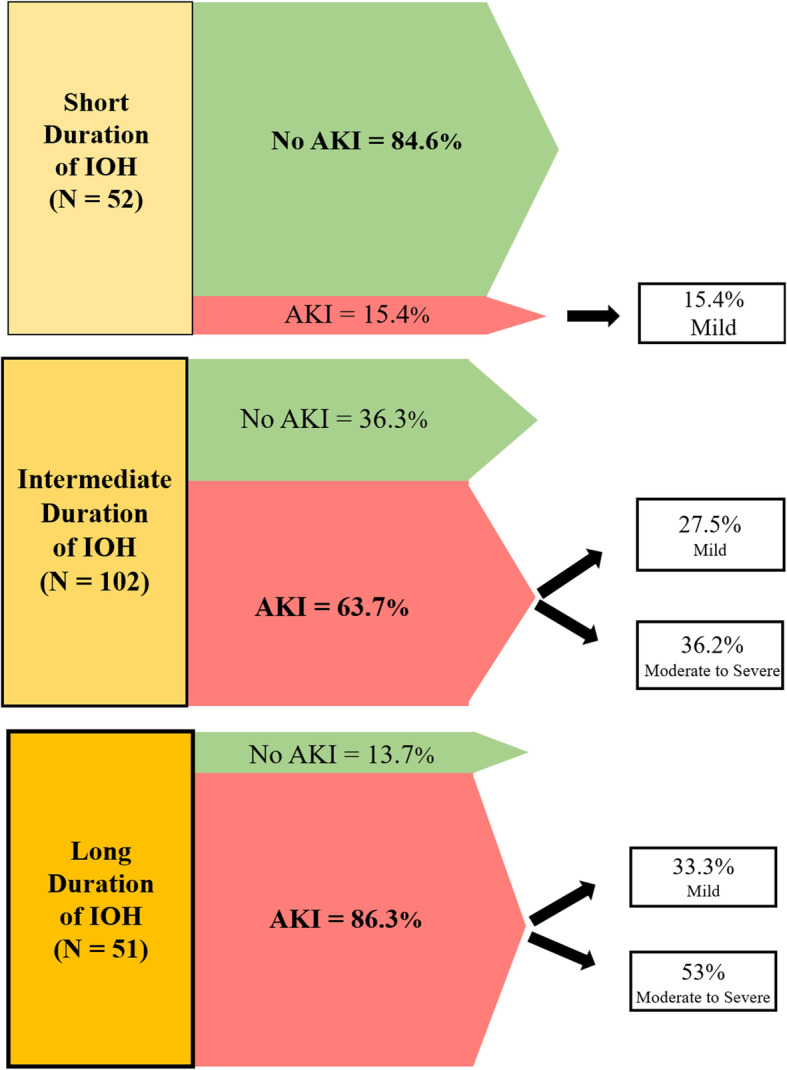
Of the 205 patients who met our inclusion criteria, 117 (57.1%) developed AKI. Fifty-two (25%), 102 (50%) and 51 (25%) patients had short, intermediate and long duration of IOH respectively. In multivariate analysis, IOH was independently associated with an increased risk of AKI (adjusted odds ratio [OR] 1.05; 95%CI 1.02-1.09; P < 0.001). Compared to "short duration" of IOH, "intermediate duration" was associated with a 10-fold increased risk of developing AKI (OR 9.7; 95%CI 4.1-22.7; P < 0.001). "Long duration" was associated with an even greater risk of AKI compared to "short duration" (OR 34.6; 95%CI 11.5-108.6; P < 0.001).
Intraoperative hypotension is independently associated with the development of AKI after liver transplant surgery. The longer the MAP is < 65 mmHg, the higher the risk the patient will develop AKI in the immediate postoperative period, and the greater the likely severity. Anesthesiologists and surgeons must therefore make every effort to avoid IOH during surgery.
肝移植手术后常发生急性肾损伤(AKI),与显著的发病率和死亡率相关。虽然术中低血压(IOH)对接受各种非心脏手术的患者术后 AKI 的影响已得到充分证实,但在肝移植手术中研究仍不够充分。我们检验了如下假说,即 IOH 与肝移植手术后 AKI 相关。
本回顾性队列研究纳入了 2014 年至 2019 年期间除术前血肌酐>1.5mg/dl 或合并移植手术外的所有接受肝移植手术的患者。术中低血压定义为任何平均动脉压(MAP)<65mmHg,并根据 MAP<65mmHg 的病例时间百分比分为三组:“短”(第 1 四分位,<8.6%的病例时间)、“中”(第 2-3 四分位,8.6-39.5%)和“长”(第 4 四分位,>39.5%)持续时间。AKI 分期根据改良“肾脏病:改善全球预后”(KDIGO)标准进行分类。采用逻辑回归模型评估 IOH 与术后 AKI 之间的关联。模型以单变量和多个围手术期协变量的形式运行,以检验对混杂因素的稳健性。
在符合纳入标准的 205 例患者中,117 例(57.1%)发生 AKI。52 例(25%)、102 例(50%)和 51 例(25%)患者的 IOH 持续时间分别为“短”、“中”和“长”。多变量分析显示,IOH 与 AKI 风险增加独立相关(调整优势比[OR]1.05;95%CI 1.02-1.09;P<0.001)。与“短时间”的 IOH 相比,“长时间”的 IOH 发生 AKI 的风险增加了 10 倍(OR 9.7;95%CI 4.1-22.7;P<0.001)。与“短时间”的 IOH 相比,“长时间”的 IOH 发生 AKI 的风险更高(OR 34.6;95%CI 11.5-108.6;P<0.001)。
术中低血压与肝移植手术后 AKI 的发生独立相关。MAP<65mmHg 的时间越长,患者在术后即刻发生 AKI 的风险越高,严重程度越大。因此,麻醉师和外科医生必须尽一切努力避免手术期间发生 IOH。