Public Health England, Manor Farm Road, Porton Down, Salisbury, UK.
Clinical Virology, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Genome Med. 2021 Jan 11;13(1):5. doi: 10.1186/s13073-020-00811-9.
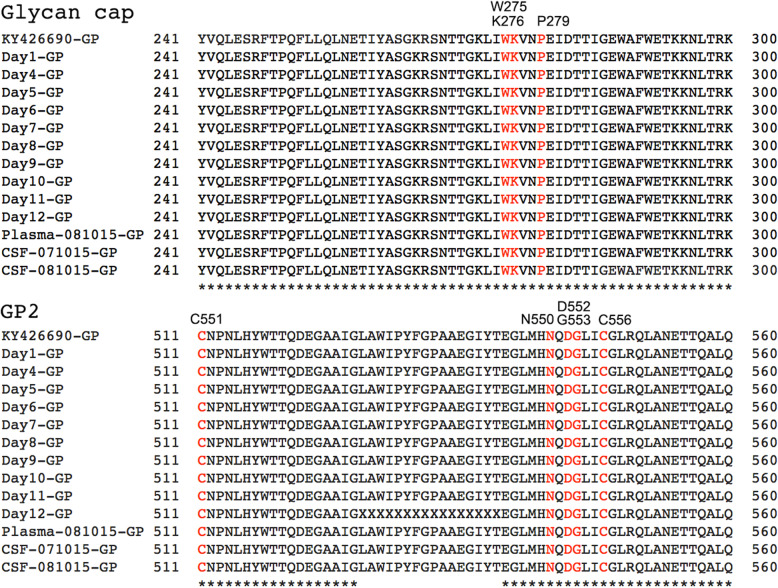
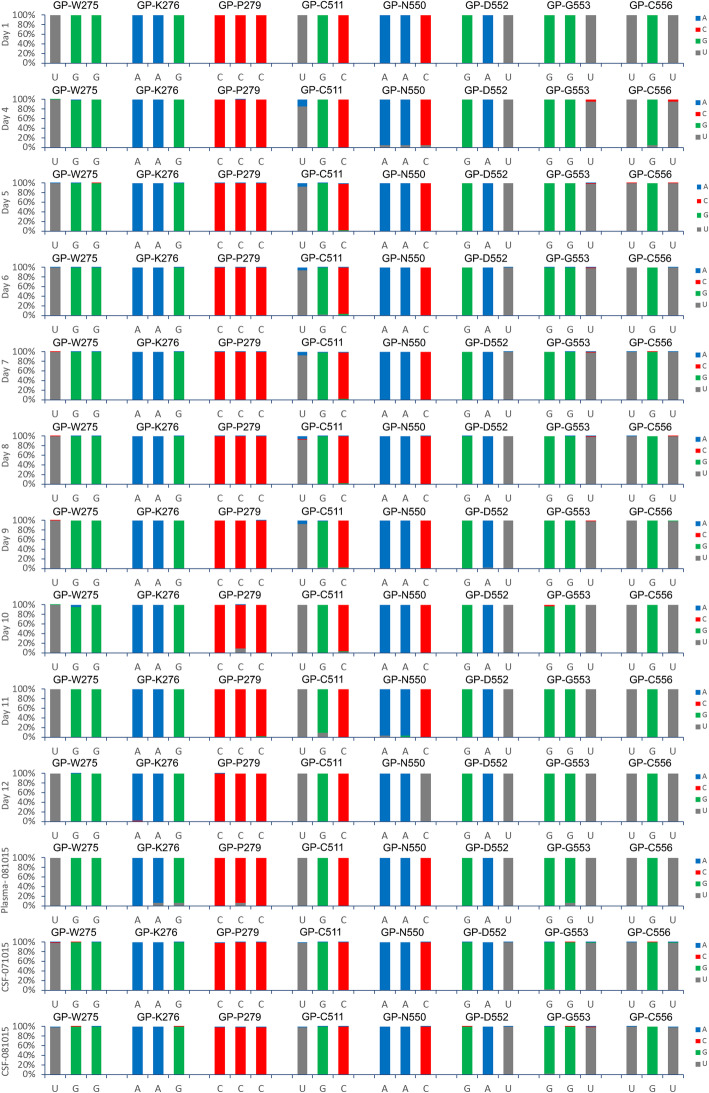
Ebola virus disease (EVD) is an often-fatal infection where the effectiveness of medical countermeasures is uncertain. During the West African outbreak (2013-2016), several patients were treated with different types of anti-viral therapies including monoclonal antibody-based cocktails that had the potential to neutralise Ebola virus (EBOV). However, at the time, the efficacy of these therapies was uncertain. Given the scale of the outbreak, several clinical phenotypes came to the forefront including the ability of the same virus to cause recrudescence in the same patient-perhaps through persisting in immune privileged sites. Several key questions remained including establishing if monoclonal antibody therapy was effective in humans with severe EVD, whether virus escape mutants were selected during treatment, and what is the potential mechanism(s) of persistence. This was made possible through longitudinal samples taken from a UK patient with EVD.
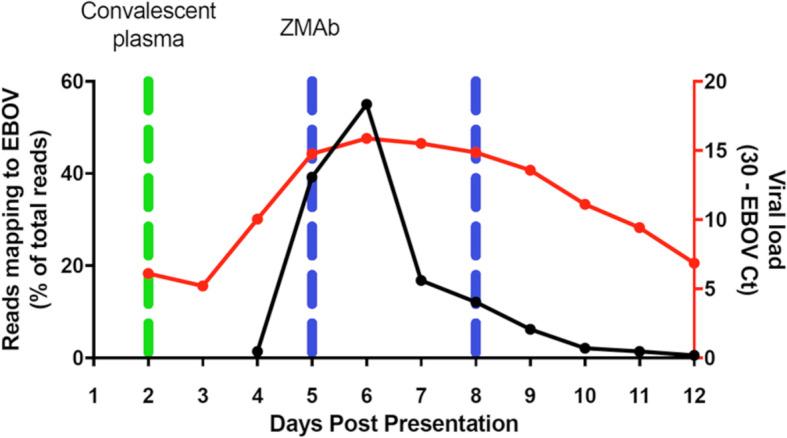
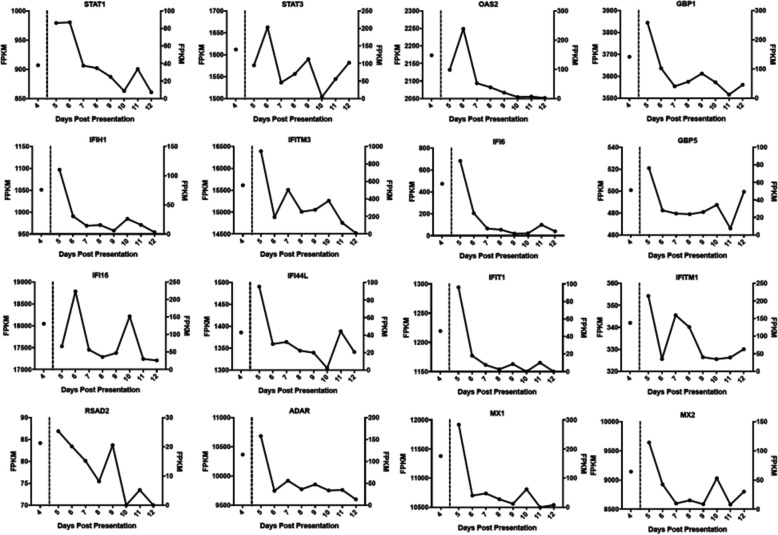
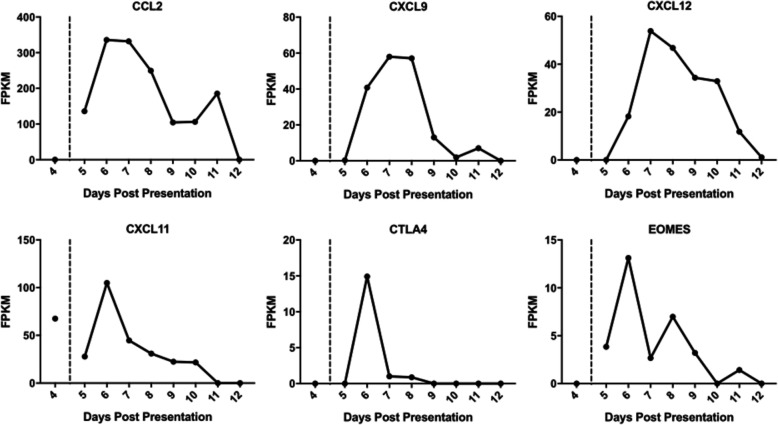
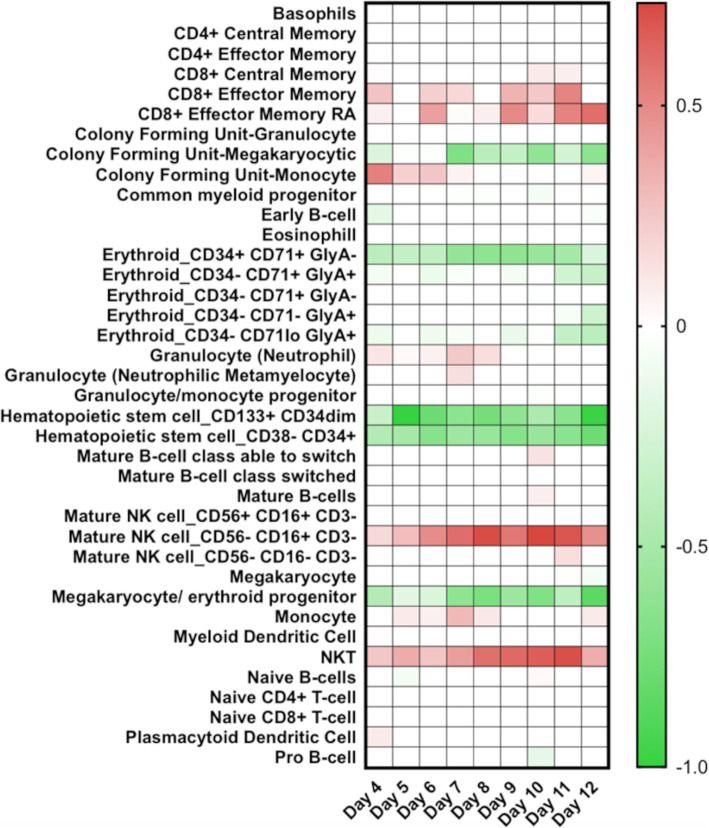
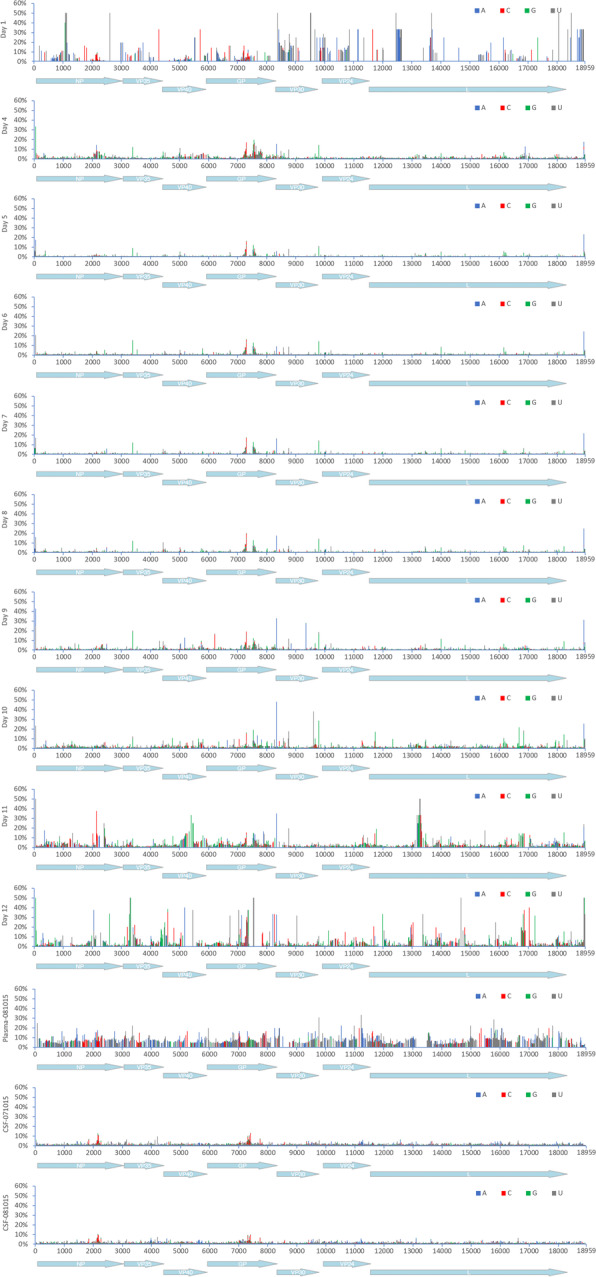
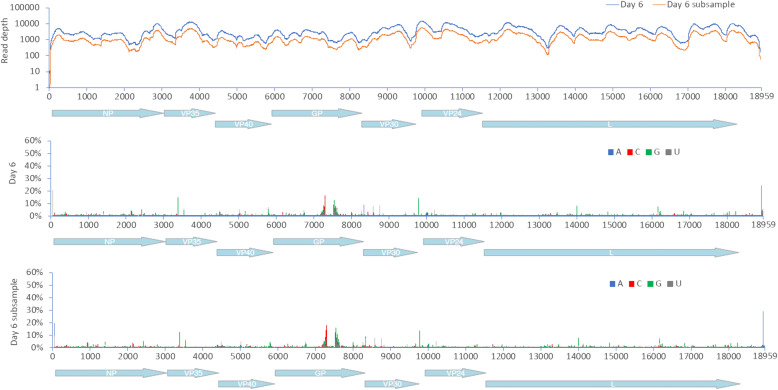
Several different sample types, plasma and cerebrospinal fluid, were collected and sequenced using Illumina-based RNAseq. Sequence reads were mapped both to EBOV and the human genome and differential gene expression analysis used to identify changes in the abundance of gene transcripts as infection progressed. Digital Cell Quantitation analysis was used to predict the immune phenotype in samples derived from blood.
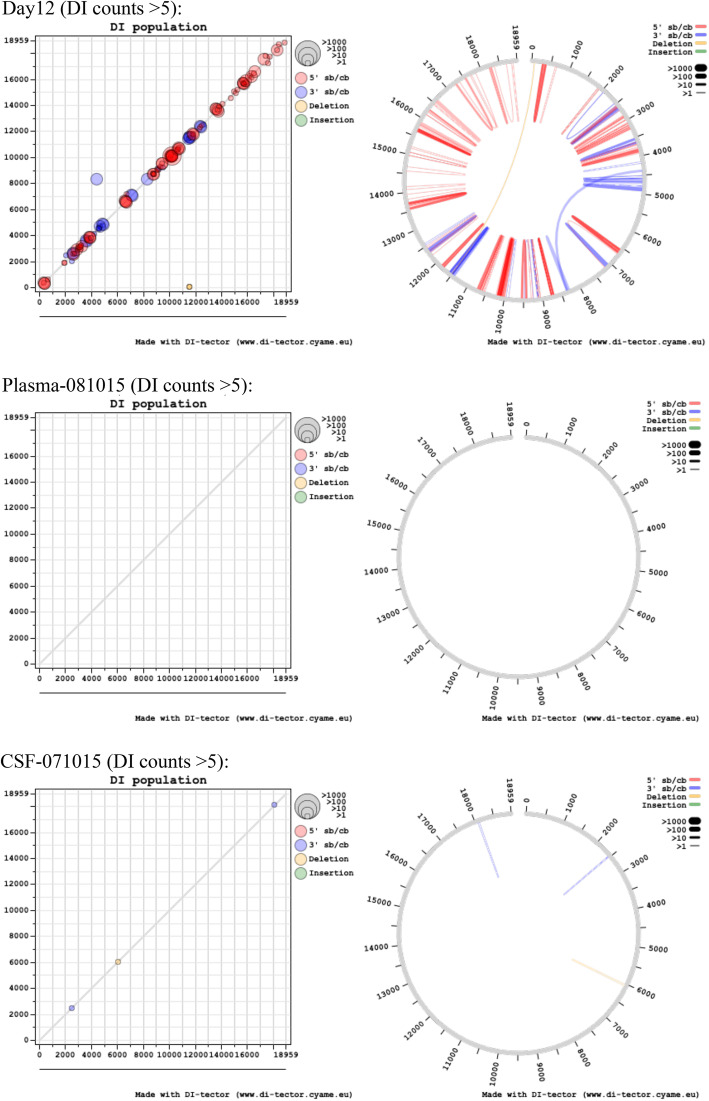
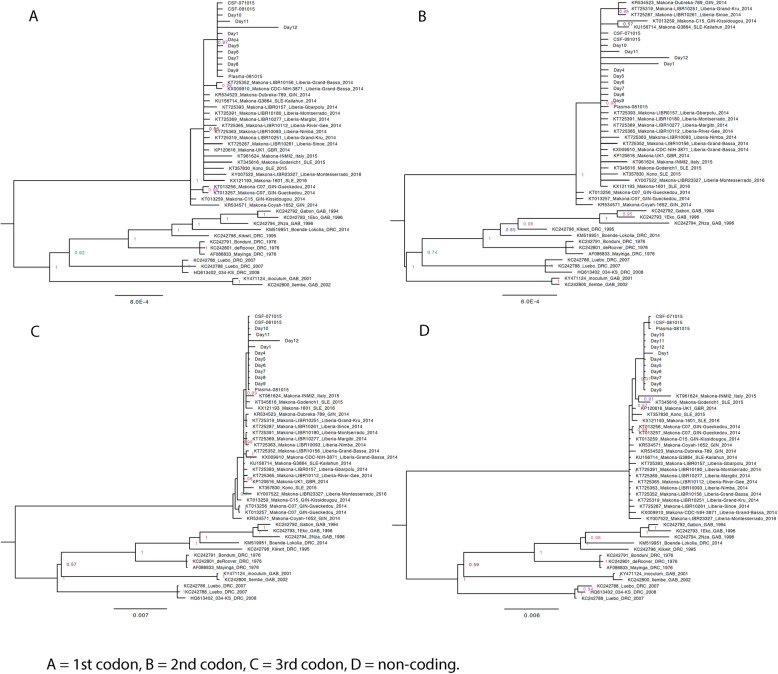
The findings were compared to equivalent data from West African patients. The study found that both virus and host markers were predictive of a fatal outcome. This suggested that the extensive supportive care, and most likely the application of the medical countermeasure ZMab (a monoclonal antibody cocktail), contributed to survival of the UK patient. The switch from progression to a 'fatal' outcome to a 'survival' outcome could be seen in both the viral and host markers. The UK patient also suffered a recrudescence infection 10 months after the initial infection. Analysis of the sequencing data indicated that the virus entered a period of reduced or minimal replication, rather than other potential mechanisms of persistence-such as defective interfering genomes.
The data showed that comprehensive supportive care and the application of medical countermeasures are worth pursuing despite an initial unfavourable prognosis.
埃博拉病毒病(EVD)是一种常致命的感染,其医学应对措施的效果不确定。在西非疫情(2013-2016 年)期间,有几名患者接受了不同类型的抗病毒治疗,包括有可能中和埃博拉病毒(EBOV)的基于单克隆抗体的鸡尾酒疗法。然而,当时这些疗法的疗效尚不确定。鉴于疫情规模,出现了几种临床表型,包括同一病毒在同一患者体内复发的能力——可能是通过在免疫特权部位持续存在。仍有几个关键问题悬而未决,包括确定单克隆抗体疗法是否对严重埃博拉病毒病患者有效,治疗过程中是否选择了病毒逃逸突变体,以及持续性的潜在机制。这是通过对一名患有埃博拉病毒病的英国患者进行的纵向样本实现的。
采集了几种不同的样本类型,包括血浆和脑脊液,并用 Illumina 基于 RNAseq 的方法进行了测序。将序列读取映射到 EBOV 和人类基因组上,并使用差异基因表达分析来识别感染进展过程中基因转录本丰度的变化。数字细胞定量分析用于预测来自血液样本的免疫表型。
将这些发现与来自西非患者的等效数据进行了比较。研究发现,病毒和宿主标志物均具有预测致命结局的能力。这表明,广泛的支持性护理,最有可能是应用了医学应对措施 ZMab(一种单克隆抗体鸡尾酒),促成了英国患者的存活。从进展到“致命”结局再到“存活”结局的转变,在病毒和宿主标志物中都可以看到。这名英国患者在初次感染 10 个月后也发生了再感染。对测序数据的分析表明,病毒进入了复制减少或最小的时期,而不是持续性的其他潜在机制,如缺陷干扰基因组。
数据表明,尽管最初的预后不佳,但全面的支持性护理和应用医学应对措施是值得的。