1Department of Intensive Care, Amsterdam University Medical Centers, Location Academic Medical Center, Amsterdam, The Netherlands.
2Mahidol-Oxford Tropical Medicine Research Unit (MORU), Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Am J Trop Med Hyg. 2021 Jan 11;104(3):1022-1033. doi: 10.4269/ajtmh.20-1177.
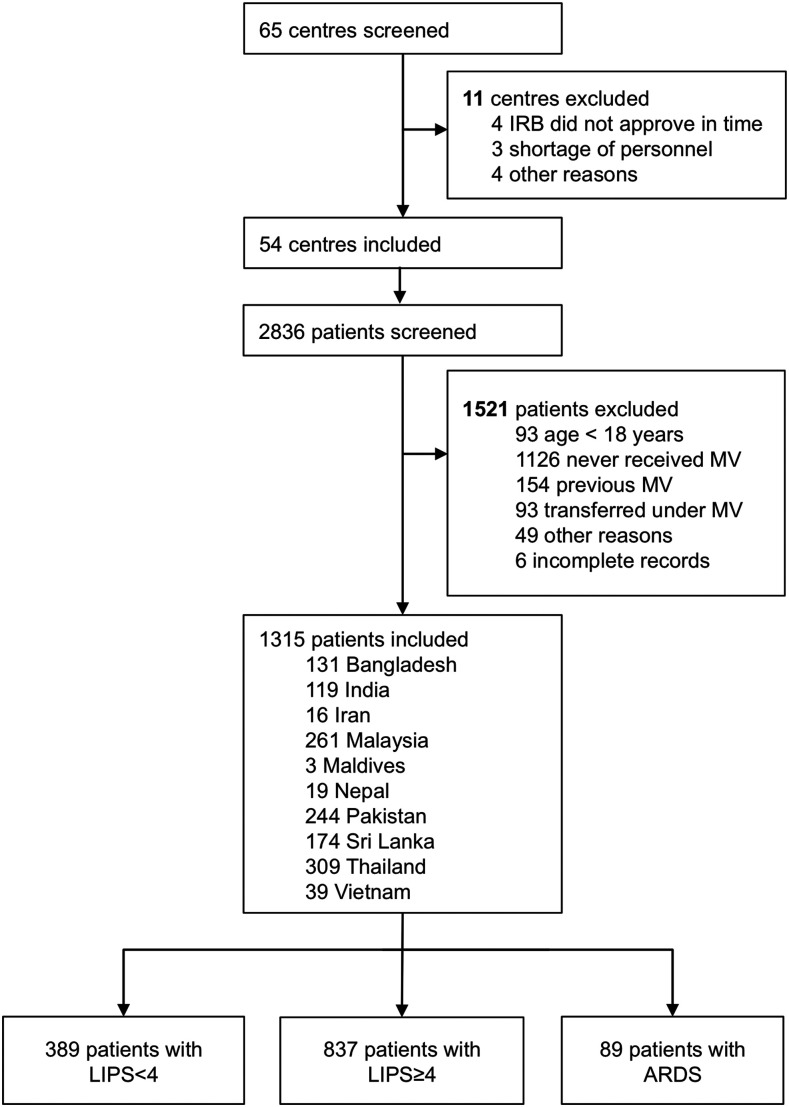
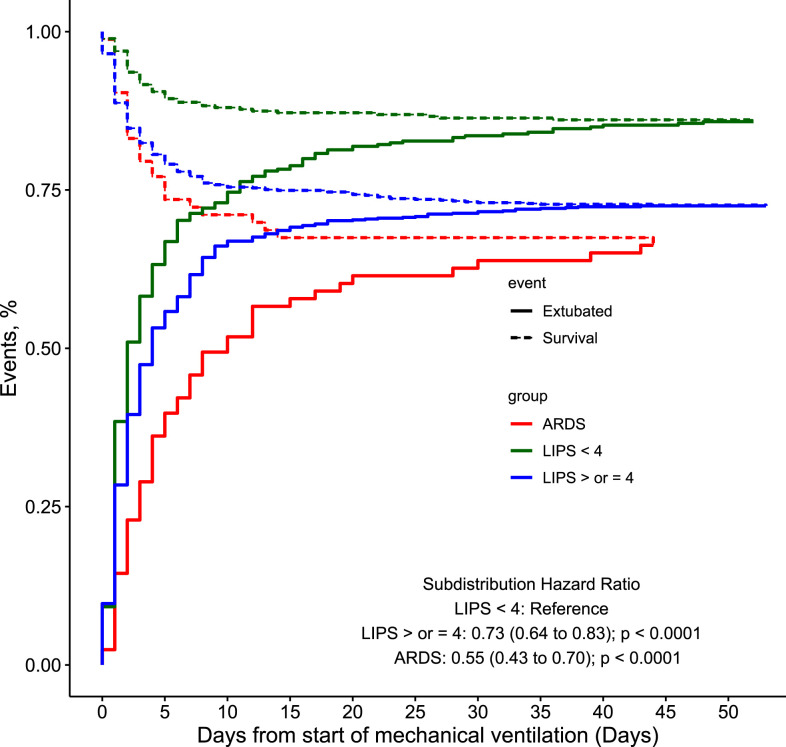
Epidemiology, ventilator management, and outcome in patients receiving invasive ventilation in intensive care units (ICUs) in middle-income countries are largely unknown. PRactice of VENTilation in Middle-income Countries is an international multicenter 4-week observational study of invasively ventilated adult patients in 54 ICUs from 10 Asian countries conducted in 2017/18. Study outcomes included major ventilator settings (including tidal volume [V T ] and positive end-expiratory pressure [PEEP]); the proportion of patients at risk for acute respiratory distress syndrome (ARDS), according to the lung injury prediction score (LIPS), or with ARDS; the incidence of pulmonary complications; and ICU mortality. In 1,315 patients included, median V T was similar in patients with LIPS < 4 and patients with LIPS ≥ 4, but lower in patients with ARDS (7.90 [6.8-8.9], 8.0 [6.8-9.2], and 7.0 [5.8-8.4] mL/kg Predicted body weight; P = 0.0001). Median PEEP was similar in patients with LIPS < 4 and LIPS ≥ 4, but higher in patients with ARDS (five [5-7], five [5-8], and 10 [5-12] cmH2O; P < 0.0001). The proportions of patients with LIPS ≥ 4 or with ARDS were 68% (95% CI: 66-71) and 7% (95% CI: 6-8), respectively. Pulmonary complications increased stepwise from patients with LIPS < 4 to patients with LIPS ≥ 4 and patients with ARDS (19%, 21%, and 38% respectively; P = 0.0002), with a similar trend in ICU mortality (17%, 34%, and 45% respectively; P < 0.0001). The capacity of the LIPS to predict development of ARDS was poor (receiver operating characteristic [ROC] area under the curve [AUC] of 0.62, 95% CI: 0.54-0.70). In Asian middle-income countries, where two-thirds of ventilated patients are at risk for ARDS according to the LIPS and pulmonary complications are frequent, setting of V T is globally in line with current recommendations.
在中低收入国家的重症监护病房(ICU)中,接受有创通气的患者的流行病学、通气管理和结局在很大程度上尚不清楚。中低收入国家的通气实践(PRactice of VENTilation in Middle-income Countries,PROVENT)是一项国际性、多中心、观察性研究,纳入了 2017/18 年期间来自亚洲 10 个国家的 54 个 ICU 中 1315 例接受有创通气的成年患者。研究结局包括主要通气设置(包括潮气量[V T ]和呼气末正压[PEEP]);根据肺损伤预测评分(LIPS)预测有急性呼吸窘迫综合征(ARDS)风险或患有 ARDS 的患者比例;肺部并发症发生率;以及 ICU 死亡率。在纳入的 1315 例患者中,LIPS<4 的患者和 LIPS≥4 的患者的 V T 中位数相似,但 ARDS 患者的 V T 较低(分别为 7.90[6.8-8.9]、8.0[6.8-9.2]和 7.0[5.8-8.4]mL/kg 预测体重;P=0.0001)。LIPS<4 的患者和 LIPS≥4 的患者的 PEEP 中位数相似,但 ARDS 患者的 PEEP 较高(分别为 5[5-7]、5[5-8]和 10[5-12]cmH2O;P<0.0001)。LIPS≥4 或 ARDS 的患者比例分别为 68%(95%CI:66-71)和 7%(95%CI:6-8)。肺部并发症发生率逐渐升高,依次为 LIPS<4 的患者、LIPS≥4 的患者和 ARDS 患者(分别为 19%、21%和 38%;P=0.0002),ICU 死亡率也呈现类似趋势(分别为 17%、34%和 45%;P<0.0001)。LIPS 预测 ARDS 发生的能力较差(ROC 曲线下面积[AUC]为 0.62,95%CI:0.54-0.70)。在亚洲中低收入国家,根据 LIPS,三分之二的接受通气的患者有患 ARDS 的风险,肺部并发症较为常见,V T 的设定与当前的推荐一致。