Department of Intensive Care, Amsterdam University Medical Centers, Academic Medical Center, Amsterdam, Netherlands; Mahidol-Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand; Section of Operative Research, Doctors with Africa, CUAMM, Padova, Italy; Department of Intensive Care, Miulli Regional General Hospital, Acquaviva delle Fonti, Bari, Italy.
Department of Intensive Care, Amsterdam University Medical Centers, Academic Medical Center, Amsterdam, Netherlands.
Lancet Glob Health. 2022 Feb;10(2):e227-e235. doi: 10.1016/S2214-109X(21)00485-X. Epub 2021 Dec 13.
Geoeconomic variations in epidemiology, the practice of ventilation, and outcome in invasively ventilated intensive care unit (ICU) patients without acute respiratory distress syndrome (ARDS) remain unexplored. In this analysis we aim to address these gaps using individual patient data of four large observational studies.
In this pooled analysis we harmonised individual patient data from the ERICC, LUNG SAFE, PRoVENT, and PRoVENT-iMiC prospective observational studies, which were conducted from June, 2011, to December, 2018, in 534 ICUs in 54 countries. We used the 2016 World Bank classification to define two geoeconomic regions: middle-income countries (MICs) and high-income countries (HICs). ARDS was defined according to the Berlin criteria. Descriptive statistics were used to compare patients in MICs versus HICs. The primary outcome was the use of low tidal volume ventilation (LTVV) for the first 3 days of mechanical ventilation. Secondary outcomes were key ventilation parameters (tidal volume size, positive end-expiratory pressure, fraction of inspired oxygen, peak pressure, plateau pressure, driving pressure, and respiratory rate), patient characteristics, the risk for and actual development of acute respiratory distress syndrome after the first day of ventilation, duration of ventilation, ICU length of stay, and ICU mortality.
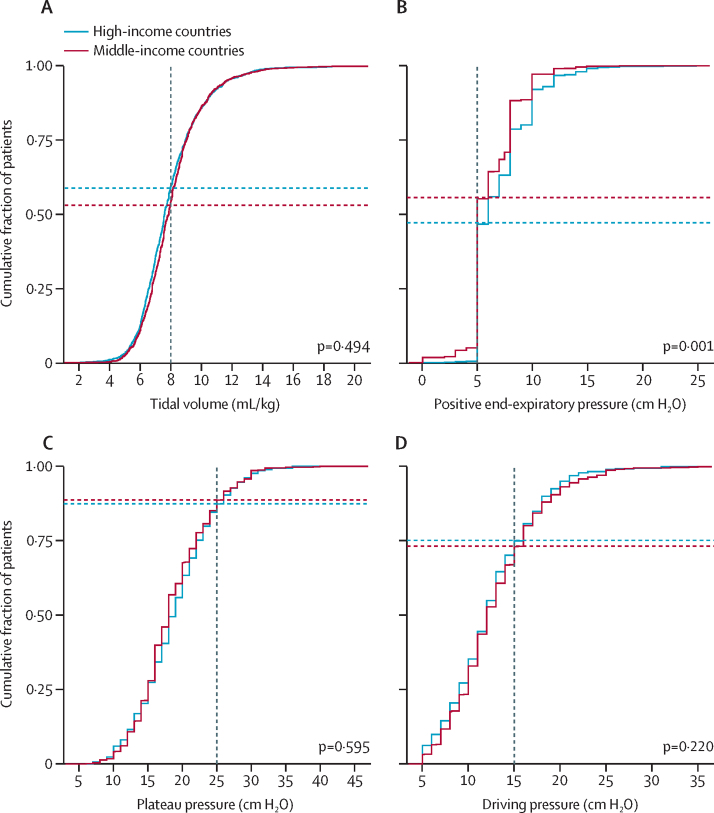
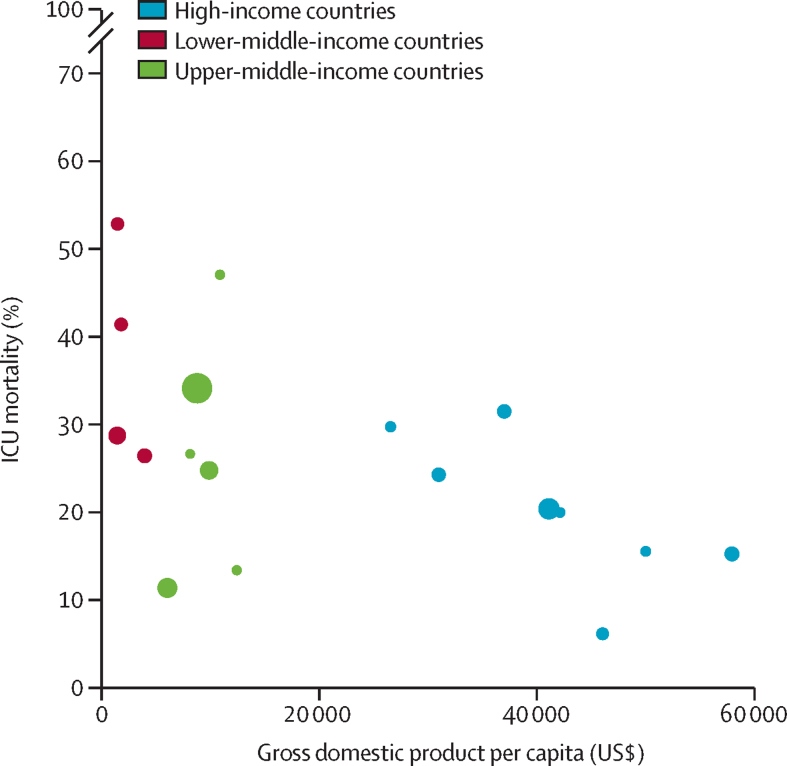
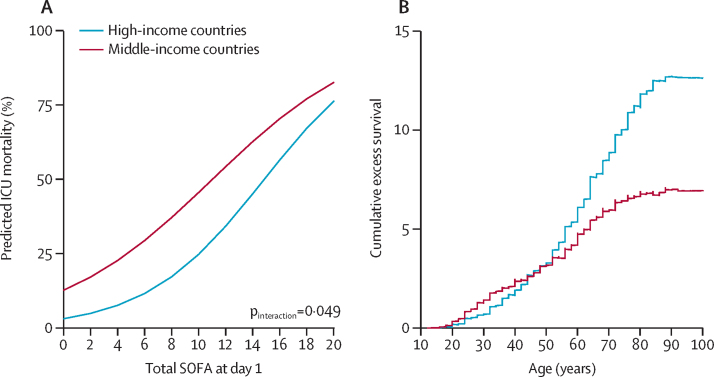
Of the 7608 patients included in the original studies, this analysis included 3852 patients without ARDS, of whom 2345 were from MICs and 1507 were from HICs. Patients in MICs were younger, shorter and with a slightly lower body-mass index, more often had diabetes and active cancer, but less often chronic obstructive pulmonary disease and heart failure than patients from HICs. Sequential organ failure assessment scores were similar in MICs and HICs. Use of LTVV in MICs and HICs was comparable (42·4% vs 44·2%; absolute difference -1·69 [-9·58 to 6·11] p=0·67; data available in 3174 [82%] of 3852 patients). The median applied positive end expiratory pressure was lower in MICs than in HICs (5 [IQR 5-8] vs 6 [5-8] cm HO; p=0·0011). ICU mortality was higher in MICs than in HICs (30·5% vs 19·9%; p=0·0004; adjusted effect 16·41% [95% CI 9·52-23·52]; p<0·0001) and was inversely associated with gross domestic product (adjusted odds ratio for a US$10 000 increase per capita 0·80 [95% CI 0·75-0·86]; p<0·0001).
Despite similar disease severity and ventilation management, ICU mortality in patients without ARDS is higher in MICs than in HICs, with a strong association with country-level economic status.
No funding.
在没有急性呼吸窘迫综合征(ARDS)的接受有创机械通气的重症监护病房(ICU)患者中,流行病学、通气实践和结局的地缘经济学差异仍未得到探索。在本分析中,我们旨在使用四项大型观察性研究的个体患者数据来解决这些差距。
在这项汇总分析中,我们对 ERICC、LUNG SAFE、PRoVENT 和 PRoVENT-iMiC 前瞻性观察性研究的个体患者数据进行了协调,这些研究于 2011 年 6 月至 2018 年 12 月在 54 个国家的 534 个 ICU 中进行。我们使用 2016 年世界银行分类来定义两个地缘经济区域:中等收入国家(MICs)和高收入国家(HICs)。ARDS 根据柏林标准定义。使用描述性统计数据比较 MICs 和 HICs 中的患者。主要结局是在前 3 天机械通气期间使用低潮气量通气(LTVV)。次要结局是关键通气参数(潮气量大小、呼气末正压、吸入氧分数、峰压、平台压、驱动压和呼吸频率)、患者特征、ARDS 风险和实际发生以及通气持续时间、ICU 住院时间和 ICU 死亡率。
在原始研究纳入的 7608 名患者中,本分析纳入了 3852 名无 ARDS 的患者,其中 2345 名来自 MICs,1507 名来自 HICs。MICs 中的患者年龄较小,身材较矮,体重指数略低,更常患有糖尿病和活动性癌症,但患有慢性阻塞性肺疾病和心力衰竭的比例较低。序贯器官衰竭评估评分在 MICs 和 HICs 中相似。MICs 和 HICs 中 LTVV 的使用情况相似(42.4% vs 44.2%;绝对差值-1.69[-9.58 至 6.11];p=0.67;在 3852 名患者中的 3174 名[82%]中提供的数据)。MICs 中应用的中位呼气末正压低于 HICs(5[IQR 5-8] vs 6[5-8]cm H2O;p=0.0011)。MICs 中的 ICU 死亡率高于 HICs(30.5% vs 19.9%;p=0.0004;调整后的效果为 16.41%[95%CI 9.52-23.52];p<0.0001),并且与国内生产总值呈负相关(人均增加 10000 美元时的调整优势比为 0.80[95%CI 0.75-0.86];p<0.0001)。
尽管疾病严重程度和通气管理相似,但无 ARDS 患者的 ICU 死亡率在 MICs 中高于 HICs,与国家经济状况有很强的关联。
无。