Department of Anaesthesiology and Intensive Care, Uniklinikum Jena, Jena, Germany.
Intensive Care Unit and Inserm CIC 1435 & UMR 1092, Dupuytren University Hospital, Limoges, France.
Crit Care. 2021 Feb 25;25(1):87. doi: 10.1186/s13054-020-03455-8.
Mortality rates for patients with ARDS remain high. We assessed temporal changes in the epidemiology and management of ARDS patients requiring invasive mechanical ventilation in European ICUs. We also investigated the association between ventilatory settings and outcome in these patients.
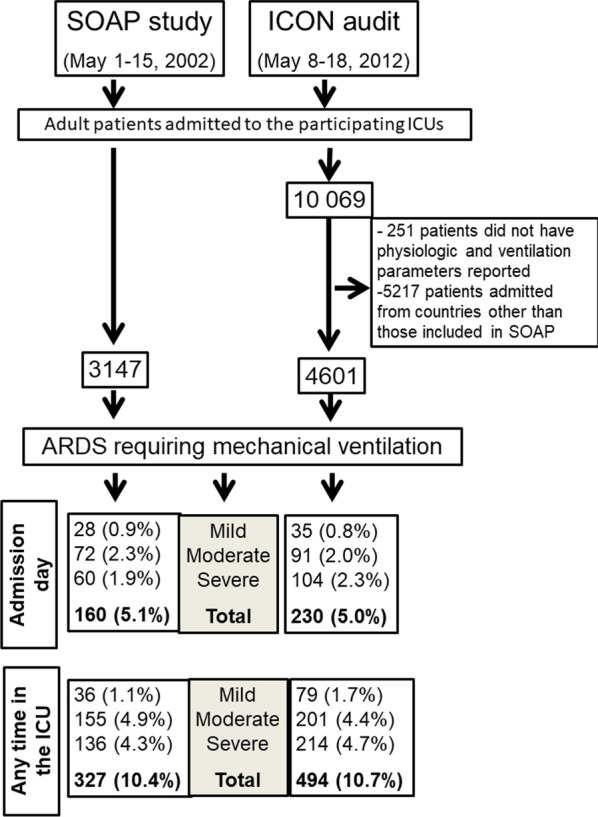
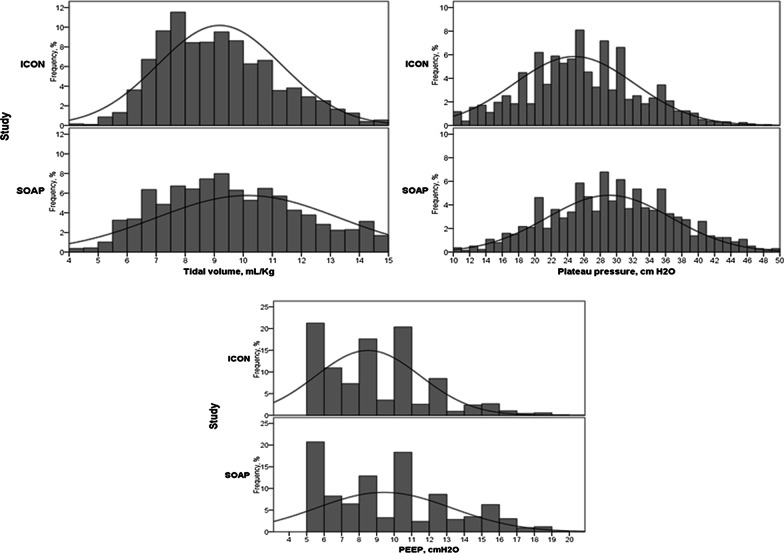
This was a post hoc analysis of two cohorts of adult ICU patients admitted between May 1-15, 2002 (SOAP study, n = 3147), and May 8-18, 2012 (ICON audit, n = 4601 admitted to ICUs in the same 24 countries as the SOAP study). ARDS was defined retrospectively using the Berlin definitions. Values of tidal volume, PEEP, plateau pressure, and FiO corresponding to the most abnormal value of arterial PO were recorded prospectively every 24 h. In both studies, patients were followed for outcome until death, hospital discharge or for 60 days.
The frequency of ARDS requiring mechanical ventilation during the ICU stay was similar in SOAP and ICON (327[10.4%] vs. 494[10.7%], p = 0.793). The diagnosis of ARDS was established at a median of 3 (IQ: 1-7) days after admission in SOAP and 2 (1-6) days in ICON. Within 24 h of diagnosis, ARDS was mild in 244 (29.7%), moderate in 388 (47.3%), and severe in 189 (23.0%) patients. In patients with ARDS, tidal volumes were lower in the later (ICON) than in the earlier (SOAP) cohort. Plateau and driving pressures were also lower in ICON than in SOAP. ICU (134[41.1%] vs 179[36.9%]) and hospital (151[46.2%] vs 212[44.4%]) mortality rates in patients with ARDS were similar in SOAP and ICON. High plateau pressure (> 29 cmHO) and driving pressure (> 14 cmHO) on the first day of mechanical ventilation but not tidal volume (> 8 ml/kg predicted body weight [PBW]) were independently associated with a higher risk of in-hospital death.
The frequency of and outcome from ARDS remained relatively stable between 2002 and 2012. Plateau pressure > 29 cmHO and driving pressure > 14 cmHO on the first day of mechanical ventilation but not tidal volume > 8 ml/kg PBW were independently associated with a higher risk of death. These data highlight the continued burden of ARDS and provide hypothesis-generating data for the design of future studies.
急性呼吸窘迫综合征(ARDS)患者的死亡率仍然很高。我们评估了在欧洲 ICU 接受有创机械通气的 ARDS 患者的流行病学和管理方面的时间变化。我们还研究了通气设置与这些患者结局之间的关系。
这是对 2002 年 5 月 1 日至 15 日(SOAP 研究,n=3147)和 2012 年 5 月 8 日至 18 日(ICON 审核,n=4601)期间入住欧洲 24 个国家与 SOAP 研究相同 ICU 的成年 ICU 患者的两个队列的事后分析。使用柏林定义回顾性定义 ARDS。记录每 24 小时动脉 PO 值最异常时的潮气量、PEEP、平台压和 FiO 值。在这两项研究中,患者的结局随访至死亡、出院或 60 天。
SOAP 和 ICON 中 ICU 期间需要机械通气的 ARDS 发生率相似(327[10.4%] vs. 494[10.7%],p=0.793)。SOAP 中 ARDS 的诊断在入院后中位 3 天(IQR:1-7)确定,而 ICON 中在第 2 天(1-6)确定。在诊断后 24 小时内,244 例(29.7%)为轻度 ARDS,388 例(47.3%)为中度 ARDS,189 例(23.0%)为重度 ARDS。在 ARDS 患者中,潮气量在较晚(ICON)队列中低于较早(SOAP)队列。平台压和驱动压在 ICON 中也低于 SOAP。SOAP 和 ICON 中 ARDS 患者的 ICU 死亡率(134[41.1%] vs. 179[36.9%])和住院死亡率(151[46.2%] vs. 212[44.4%])相似。机械通气第 1 天的高平台压(>29 cmH2O)和驱动压(>14 cmH2O)而不是潮气量(>8 ml/kg 预测体重 [PBW])与院内死亡风险增加独立相关。
2002 年至 2012 年间,ARDS 的发生率和结局相对稳定。机械通气第 1 天的平台压>29 cmH2O 和驱动压>14 cmH2O 而不是潮气量>8 ml/kg PBW 与死亡风险增加独立相关。这些数据突出了 ARDS 的持续负担,并为未来研究的设计提供了产生假设的数据。