TIMI Study Group, Division of Cardiovascular Medicine, Department of Medicine (N.A.M., G.E.M.M., Y.G., F.K.K., R.P.G., B.M.S., E.B., M.S.S., C.T.R.), Brigham and Women's Hospital, Harvard Medical School, Boston, MA.
CPC Clinical Research, Cardiovascular Division, Department of Medicine, University of Colorado School of Medicine, Aurora (M.P.B.).
Circ Genom Precis Med. 2021 Feb;14(1):e003006. doi: 10.1161/CIRCGEN.120.003006. Epub 2021 Jan 12.
Venous thromboembolism (VTE) is a major cause of cardiovascular morbidity and mortality and has a known genetic contribution. We tested the performance of a genetic risk score for its ability to predict VTE in 3 cohorts of patients with cardiometabolic disease.
We included patients from the FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Patients With Elevated Risk), PEGASUS-TIMI 54 (Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin), and SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus) trials (history of a major atherosclerotic cardiovascular event, myocardial infarction, and diabetes, respectively) who consented for genetic testing and were not on baseline anticoagulation. We calculated a VTE genetic risk score based on 297 single nucleotide polymorphisms with established genome-wide significance. Patients were divided into tertiles of genetic risk. Cox proportional hazards models were used to calculate hazard ratios for VTE across genetic risk groups. The polygenic risk score was compared with available clinical risk factors (age, obesity, smoking, history of heart failure, and diabetes) and common monogenic mutations.
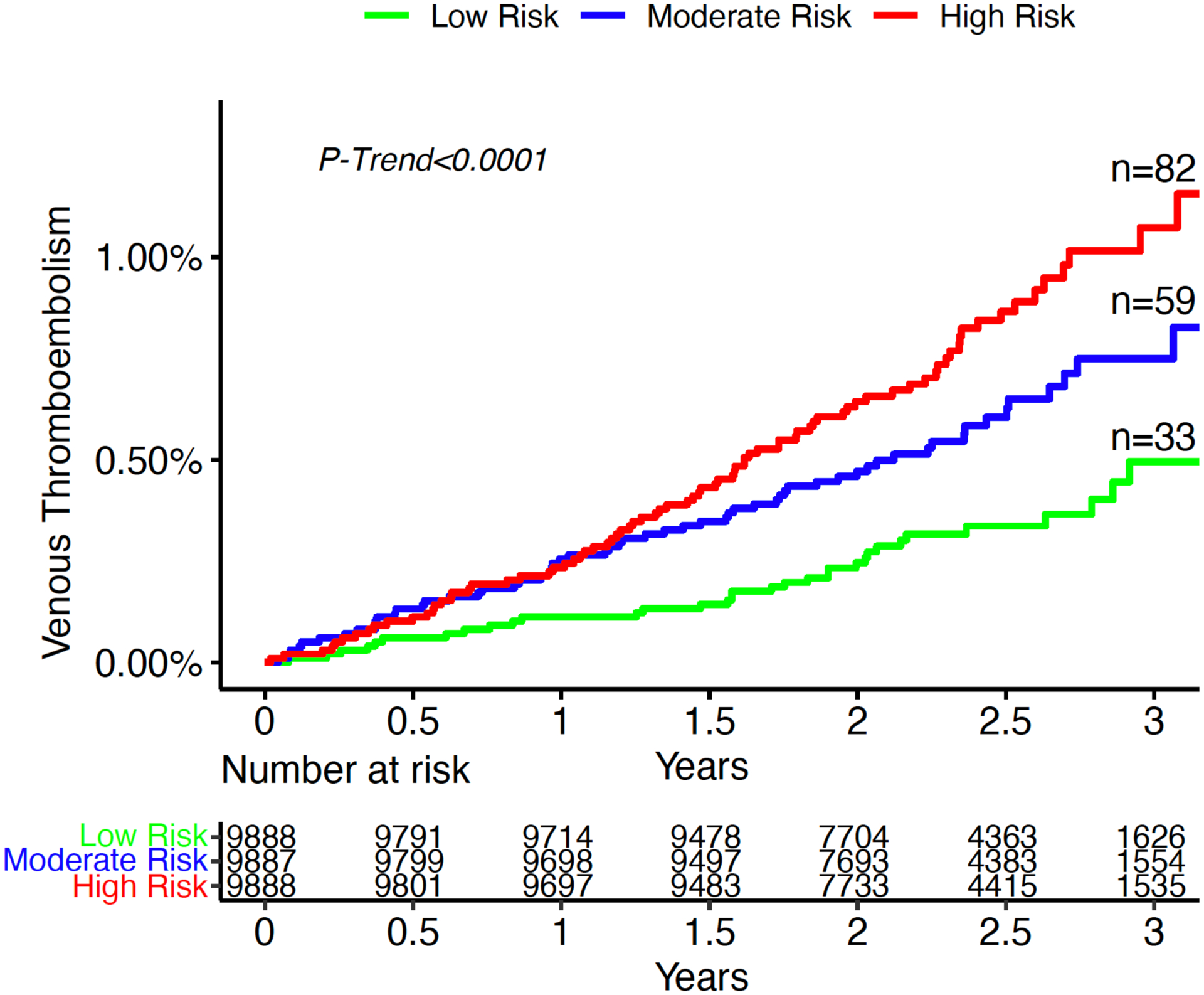
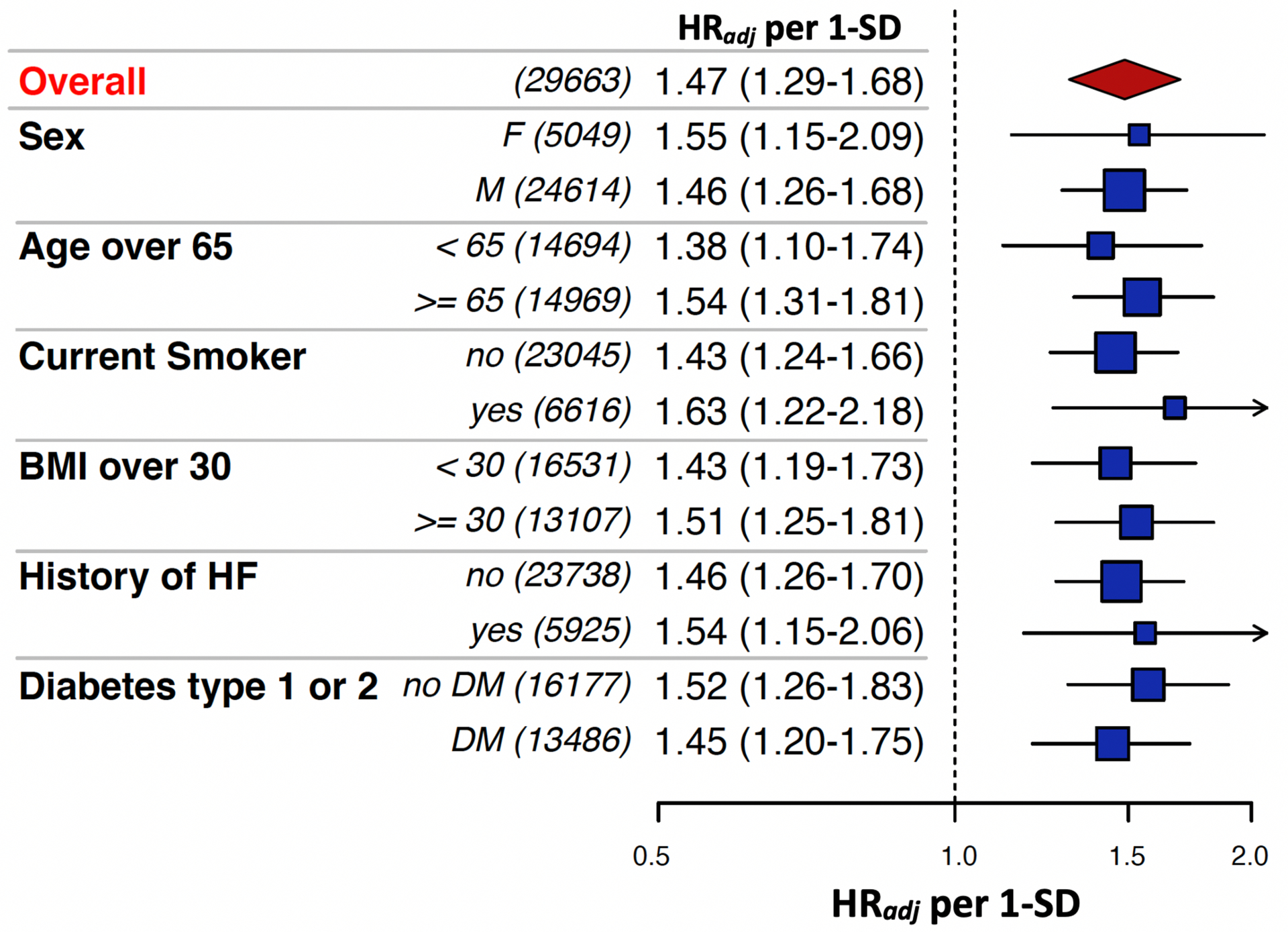
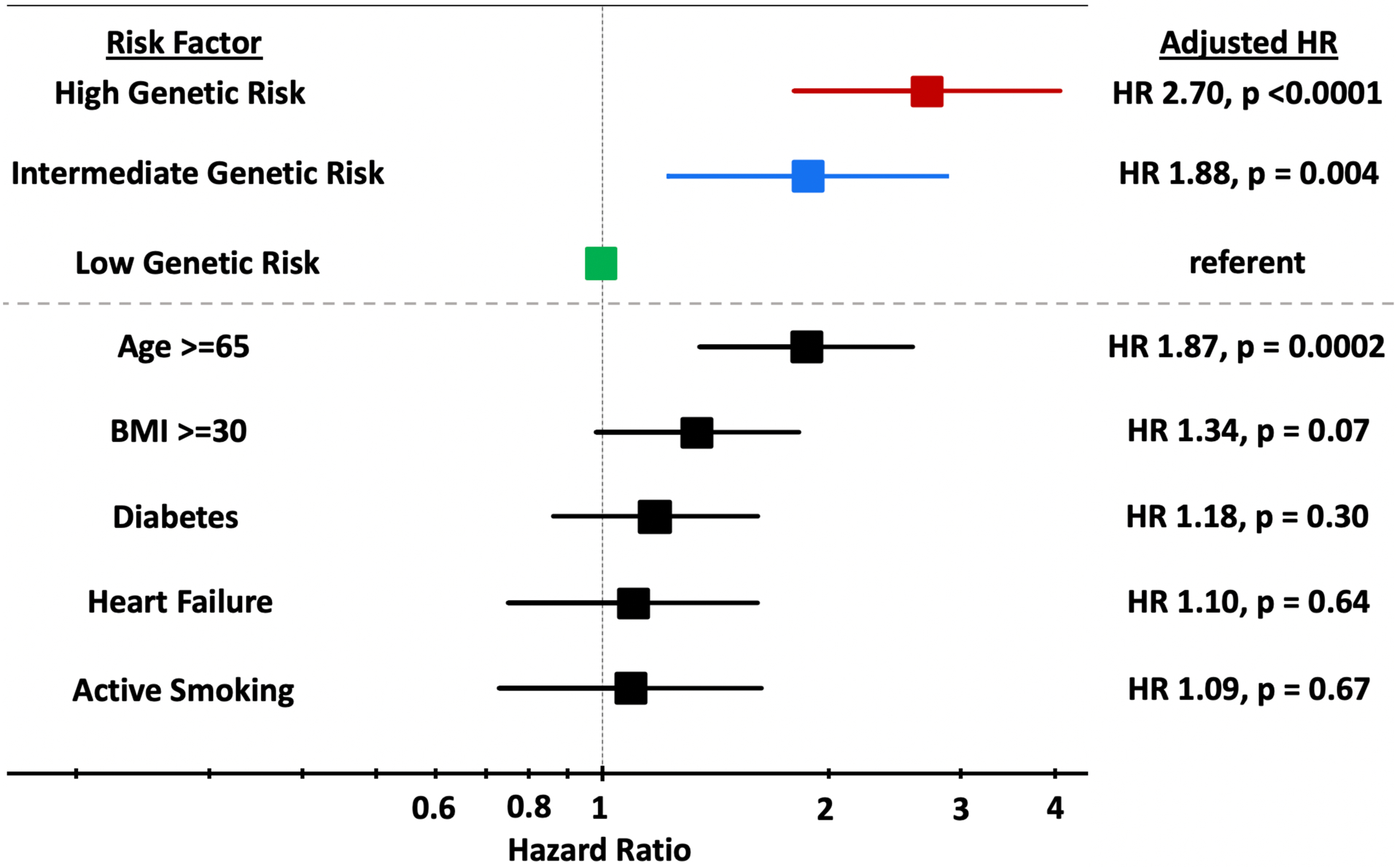
A total of 29 663 patients were included in the analysis with a median follow-up of 2.4 years, of whom 174 had a VTE event. There was a significantly increased gradient of risk across VTE genetic risk tertiles (-trend <0.0001). After adjustment for clinical risk factors, patients in the intermediate and high genetic risk groups had a 1.88-fold (95% CI, 1.23-2.89; =0.004) and 2.70-fold (95% CI, 1.81-4.06; <0.0001) higher risk of VTE compared with patients with low genetic risk. In a continuous model adjusted for clinical risk factors, each standard deviation increase in the genetic risk score was associated with a 47% (95% CI, 29-68) increased risk of VTE (<0.0001).
In a broad spectrum of patients with cardiometabolic disease, a polygenic risk score is a strong, independent predictor of VTE after accounting for available clinical risk factors, identifying 1/3 of patients who have a risk of VTE comparable to that seen with established monogenic thrombophilia.
静脉血栓栓塞症(VTE)是心血管发病率和死亡率的主要原因,其具有已知的遗传贡献。我们测试了遗传风险评分预测患有心血管代谢疾病的 3 组患者 VTE 的能力。
我们纳入了 FOURIER(使用 PCSK9 抑制剂在高风险患者中进一步心血管结局研究)、PEGASUS-TIMI 54(使用替格瑞洛与安慰剂在阿司匹林背景下预防有既往心肌梗死的患者心血管事件)和 SAVOR-TIMI 53(糖尿病患者的 saxagliptin 血管结局记录)试验(分别为主要动脉粥样硬化性心血管事件、心肌梗死和糖尿病的病史)的患者,这些患者同意进行基因检测且基线时未接受抗凝治疗。我们基于 297 个具有全基因组显著意义的单核苷酸多态性计算了 VTE 遗传风险评分。患者按遗传风险分为三分位组。Cox 比例风险模型用于计算遗传风险组之间 VTE 的风险比。多基因风险评分与现有的临床危险因素(年龄、肥胖、吸烟、心力衰竭史和糖尿病)和常见的单基因突变进行了比较。
共纳入 29663 名患者进行分析,中位随访时间为 2.4 年,其中 174 名患者发生 VTE 事件。VTE 遗传风险三分位组之间存在显著的风险梯度(趋势<0.0001)。在调整临床危险因素后,中危和高危遗传风险组的患者 VTE 风险分别为低遗传风险组的 1.88 倍(95%CI,1.23-2.89;=0.004)和 2.70 倍(95%CI,1.81-4.06;<0.0001)。在调整临床危险因素的连续模型中,遗传风险评分每增加一个标准差,VTE 的风险增加 47%(95%CI,29-68)(<0.0001)。
在广泛的患有心血管代谢疾病的患者中,多基因风险评分是 VTE 的强有力、独立预测因素,可在考虑到现有临床危险因素的情况下,识别出 1/3 的患者 VTE 风险与已确立的单基因易栓症相似。