Department of Obstetrics and Gynecology, University Hospital of Düsseldorf, Moorenstraße 5, 40225, Düsseldorf, Germany.
Department of Obstetrics and Gynecology, Franziskus Hospital Bielefeld, Kiskerstraße 26, 33615, Bielefeld, Nordrhein-Westfalen, Germany.
BMC Womens Health. 2021 Jan 12;21(1):23. doi: 10.1186/s12905-020-01165-5.
Since the introduction of sentinel node biopsy (SLNB) in unifocal vulvar cancer (diameter of < 4 cm) and unsuspicious groin lymph nodes, the morbidity rate of patients has significantly decreased globally. In contrast to SLNB, bilateral inguinofemoral lymphadenectomy (IFL) has been associated with increased risk of common morbidities. Current guidelines (NCCN, ESGO, RCOG, and German) recommend that in cases of unilaterally positive sentinel lymph node (SLN), bilateral IFL should be performed. However, two recent publications by Woelber et al. and Nica et al. contradict the current guideline, since a significant rate of positive non sentinel lymph nodes in IFL contralaterally was not observed [Woelber et al. 0% (p = 0/28) and Nica et al. 5.3% (p = 1/19)].
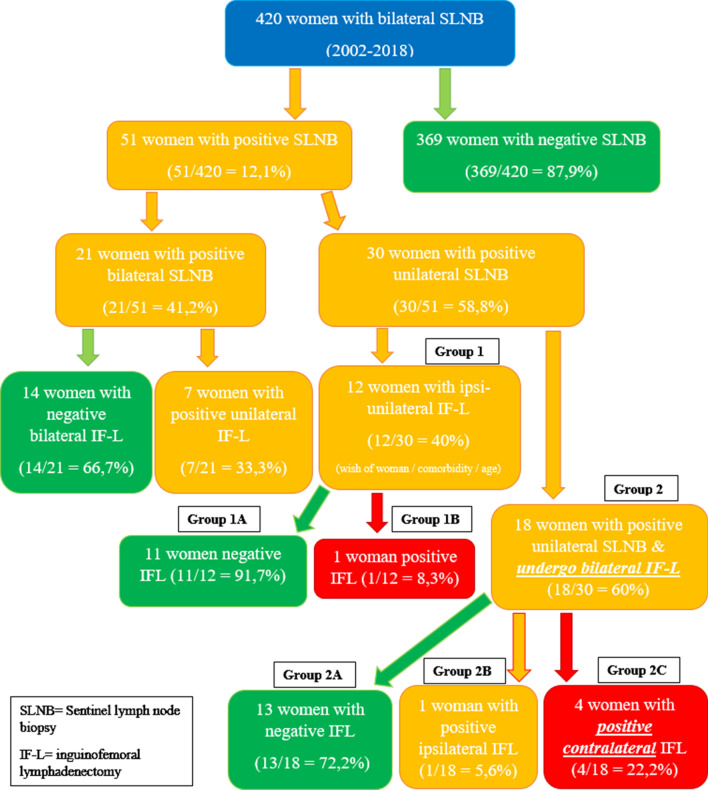
A retrospective single-center analysis conducted in the University Hospital of Dusseldorf, evaluating vulvar cancer patients treated with SLNB from 2002 to 2018.
22.2% of women (n = 4/18) were found to have contralateral IFL groin metastasis after an initial diagnosis of unilateral SLN metastasis. The depth of tumor infiltrating cells correlated significantly and positively with the rate of incidence of groin metastasis (p = 0.0038).
Current guideline for bilateral IFL should remain as the standard management. Therefore, this depth may be taken into account as an indication for bilateral IFL. The management of VC and SLNB should be performed in a high volume center with an experienced team in marking SLN and performing the adequate surgical procedure. Well conducted counseling of the patients outlining advantages but also potential oncological risks of this technique especially concerning rate of groin recurrence is critical.
自从在单灶外阴癌(直径 < 4cm)和腹股沟淋巴结无可疑转移的情况下引入前哨淋巴结活检(SLNB)以来,全球范围内患者的发病率显著降低。与 SLNB 相比,双侧腹股沟股淋巴结清扫术(IFL)会增加常见并发症的风险。目前的指南(NCCN、ESGO、RCOG 和德国)建议,对于单侧前哨淋巴结(SLN)阳性的病例,应行双侧 IFL。然而,最近 Woelber 等人和 Nica 等人的两项研究结果与当前指南相矛盾,因为在 IFL 对侧并未观察到非前哨淋巴结阳性的显著比例[Woelber 等人 0%(p=0/28)和 Nica 等人 5.3%(p=1/19)]。
这是一项在杜塞尔多夫大学医院进行的回顾性单中心分析,评估了 2002 年至 2018 年间接受 SLNB 治疗的外阴癌患者。
在初始诊断为单侧 SLN 转移后,有 22.2%(4/18)的女性发现对侧 IFL 腹股沟转移。肿瘤浸润细胞的深度与腹股沟转移的发生率呈显著正相关(p=0.0038)。
目前对于双侧 IFL 的指南仍然应该作为标准管理。因此,这一深度可能可以作为双侧 IFL 的指征。外阴癌和 SLNB 的管理应在具有经验丰富的 SLN 标记和实施适当手术团队的高容量中心进行。对患者进行良好的咨询,阐明该技术的优势,但也要特别注意腹股沟复发的潜在肿瘤学风险,这一点至关重要。