Department of Infection, Immunity and Cardiovascular Disease, University of Sheffield, Sheffield, S10 2RX, UK.
Sheffield Teaching Hospital NHS Foundation Trust, Sheffield, UK.
Sci Rep. 2021 Jan 12;11(1):617. doi: 10.1038/s41598-020-79729-6.
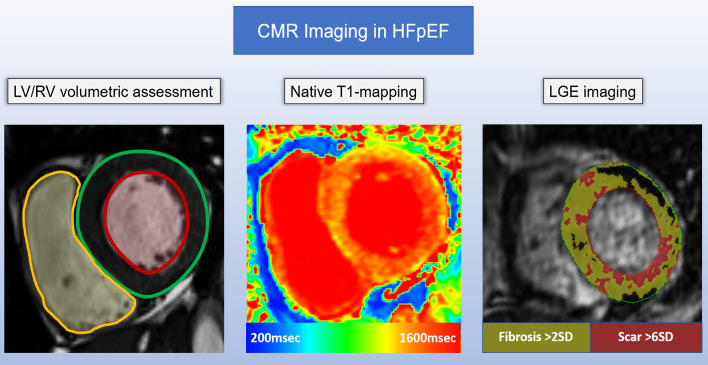
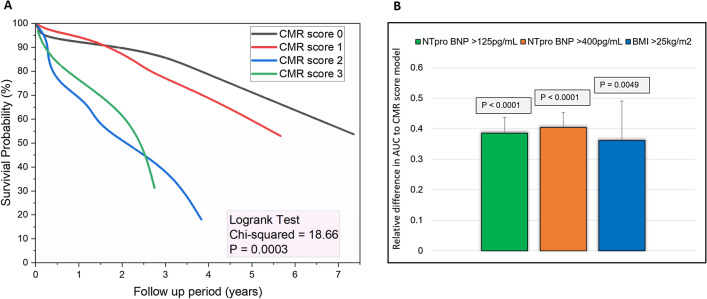
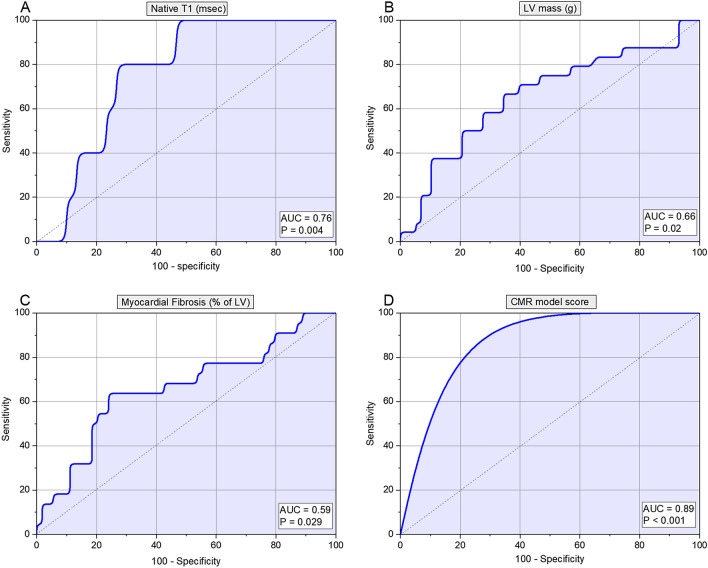
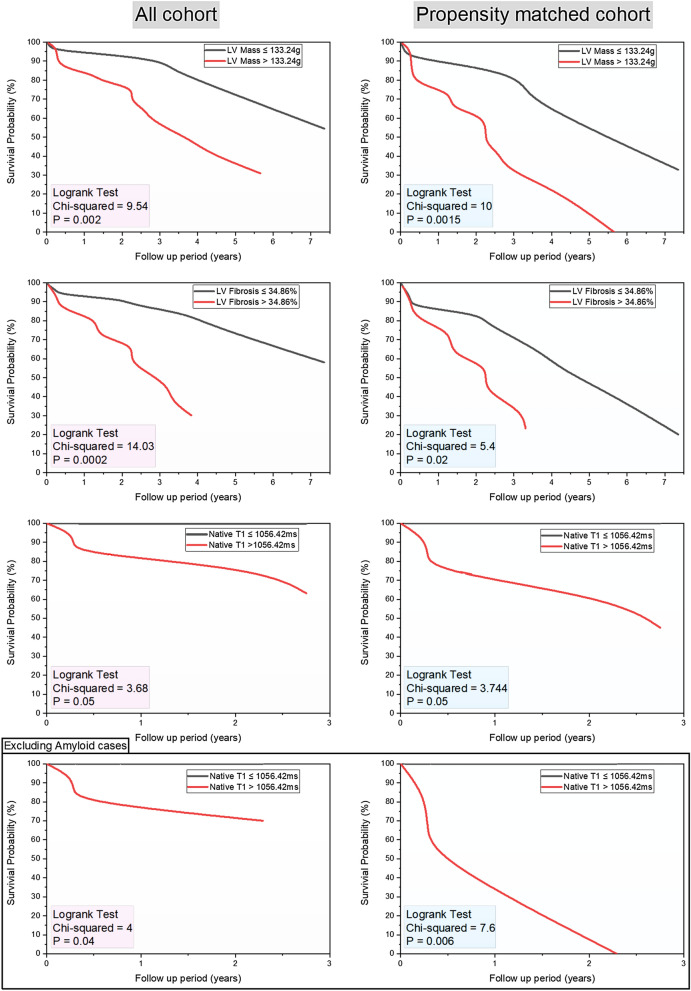
Cardiac magnetic resonance (CMR) is emerging as an important tool in the assessment of heart failure with preserved ejection fraction (HFpEF). This study sought to investigate the prognostic value of multiparametric CMR, including left and right heart volumetric assessment, native T1-mapping and LGE in HFpEF. In this retrospective study, we identified patients with HFpEF who have undergone CMR. CMR protocol included: cines, native T1-mapping and late gadolinium enhancement (LGE). The mean follow-up period was 3.2 ± 2.4 years. We identified 86 patients with HFpEF who had CMR. Of the 86 patients (85% hypertensive; 61% males; 14% cardiac amyloidosis), 27 (31%) patients died during the follow up period. From all the CMR metrics, LV mass (area under curve [AUC] 0.66, SE 0.07, 95% CI 0.54-0.76, p = 0.02), LGE fibrosis (AUC 0.59, SE 0.15, 95% CI 0.41-0.75, p = 0.03) and native T1-values (AUC 0.76, SE 0.09, 95% CI 0.58-0.88, p < 0.01) were the strongest predictors of all-cause mortality. The optimum thresholds for these were: LV mass > 133.24 g (hazard ratio [HR] 1.58, 95% CI 1.1-2.2, p < 0.01); LGE-fibrosis > 34.86% (HR 1.77, 95% CI 1.1-2.8, p = 0.01) and native T1 > 1056.42 ms (HR 2.36, 95% CI 0.9-6.4, p = 0.07). In multivariate cox regression, CMR score model comprising these three variables independently predicted mortality in HFpEF when compared to NTproBNP (HR 4 vs HR 1.65). In non-amyloid HFpEF cases, only native T1 > 1056.42 ms demonstrated higher mortality (AUC 0.833, p < 0.01). In patients with HFpEF, multiparametric CMR aids prognostication. Our results show that left ventricular fibrosis and hypertrophy quantified by CMR are associated with all-cause mortality in patients with HFpEF.
心脏磁共振(CMR)作为评估射血分数保留型心力衰竭(HFpEF)的重要工具正在兴起。本研究旨在探讨多参数 CMR 的预后价值,包括左、右心容积评估、心肌 T1 mapping 和 LGE 在 HFpEF 中的应用。
在这项回顾性研究中,我们确定了接受 CMR 的 HFpEF 患者。CMR 方案包括:电影、心肌 T1 mapping 和晚期钆增强(LGE)。平均随访时间为 3.2±2.4 年。我们共确定了 86 例接受 CMR 的 HFpEF 患者。在这 86 例患者中(85%为高血压;61%为男性;14%为心脏淀粉样变性),27 例(31%)患者在随访期间死亡。
在所有 CMR 指标中,左心室质量(曲线下面积 [AUC] 0.66,SE 0.07,95%CI 0.54-0.76,p=0.02)、LGE 纤维化(AUC 0.59,SE 0.15,95%CI 0.41-0.75,p=0.03)和心肌 T1 值(AUC 0.76,SE 0.09,95%CI 0.58-0.88,p<0.01)是全因死亡率的最强预测因子。这些指标的最佳截断值分别为:左心室质量>133.24g(危险比 [HR] 1.58,95%CI 1.1-2.2,p<0.01);LGE 纤维化>34.86%(HR 1.77,95%CI 1.1-2.8,p=0.01)和心肌 T1>1056.42ms(HR 2.36,95%CI 0.9-6.4,p=0.07)。在多变量 Cox 回归中,与 NTproBNP 相比,包含这三个变量的 CMR 评分模型可独立预测 HFpEF 患者的死亡率(HR 4 与 HR 1.65)。在非淀粉样 HFpEF 病例中,只有心肌 T1>1056.42ms 显示出更高的死亡率(AUC 0.833,p<0.01)。
在 HFpEF 患者中,多参数 CMR 有助于预后评估。我们的研究结果表明,CMR 量化的左心室纤维化和肥厚与 HFpEF 患者的全因死亡率相关。